

Global, regional, and national prevalence, incidence, mortality, and risk factors for atrial fibrillation, 1990-2017: results from the Global Burden of Disease Study 2017
- PMID: 32735316
- PMCID: PMC8557444
- DOI: 10.1093/ehjqcco/qcaa061
Global, regional, and national prevalence, incidence, mortality, and risk factors for atrial fibrillation, 1990-2017: results from the Global Burden of Disease Study 2017
Abstract
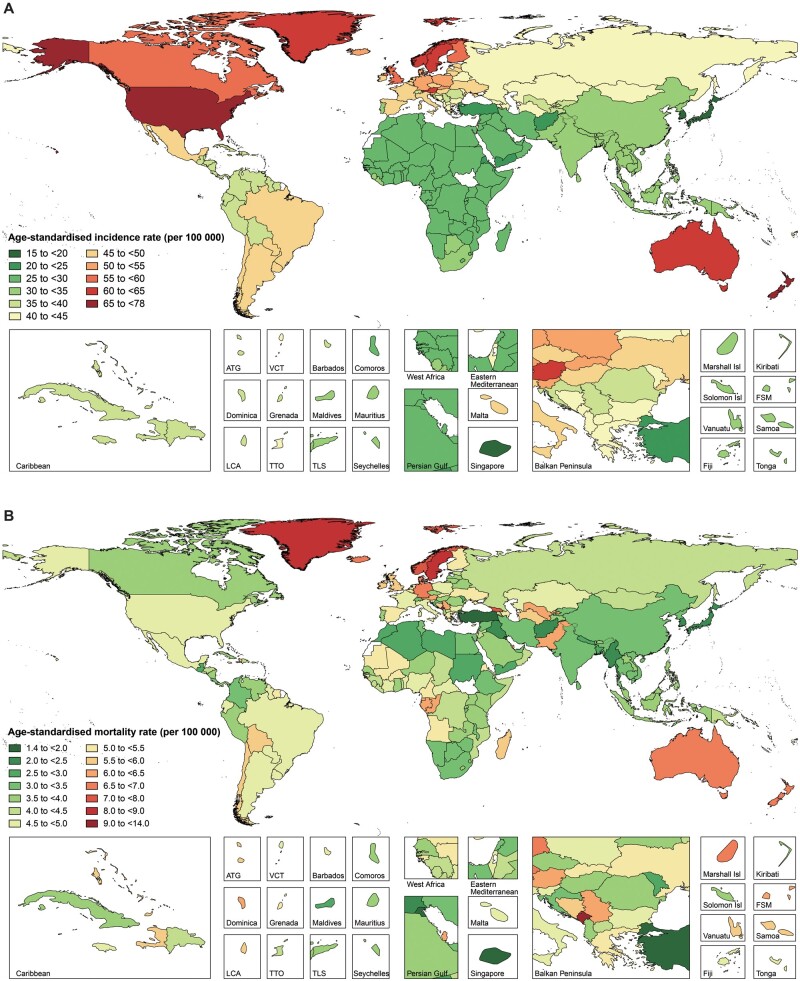
Aims: To estimate the prevalence, incidence, mortality, and risk factors for atrial fibrillation (AF) in 195 countries and territories from 1990 to 2017.
Methods and results: Following the methodologies used in the Global Burden of Disease Study 2017, the prevalence, incidence, and mortality of AF were analysed by age, sex, year, socio-demographic index (SDI), and location. The percentage contributions of major risk factors to age-standardized AF deaths were measured by population attributable fractions. In 2017, there were 37.57 million [95% uncertainty interval (UI) 32.55-42.59] prevalent cases and 3.05 million (95% UI 2.61-3.51) incident cases of AF globally, contributing to 287 241 (95% UI 276 355-304 759) deaths. The age-standardized rates of prevalent cases, incident cases, and deaths of AF in 2017 and their temporal trends from 1990 to 2017 varied significantly by SDI quintile and location. High systolic blood pressure was the leading risk factor for AF age-standardized deaths [34.3% (95% UI 27.4-41.5)] in 2017, followed by high body mass index [20.7% (95% UI 11.5-32.2)] and alcohol use [9.4% (95% UI 7.0-12.2)].
Conclusion: Our study has systematically and globally assessed the temporal trends of AF, which remains a major public heath challenge. Although AF mainly occurred in developed countries, the unfavourable trend in countries with lower SDI also deserves particular attention. More effective prevention and treatment strategies aimed at counteracting the increase in AF burden should be established in some countries.
Keywords: Atrial fibrillation; Incidence; Mortality; Prevalence; Risk factor.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures



References
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med 2002;113:359–364. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–125. - PubMed
