Economic Burden of Postoperative Neurocognitive Disorders Among US Medicare Patients
- PMID: 32735336
- PMCID: PMC7395237
- DOI: 10.1001/jamanetworkopen.2020.8931
Economic Burden of Postoperative Neurocognitive Disorders Among US Medicare Patients
Abstract
Importance: Postoperative neurocognitive disorders (PNDs) after surgical procedures are common and may be associated with increased health care expenditures.
Objective: To quantify the economic burden associated with a PND diagnosis in 1 year following surgical treatment among older patients in the United States.
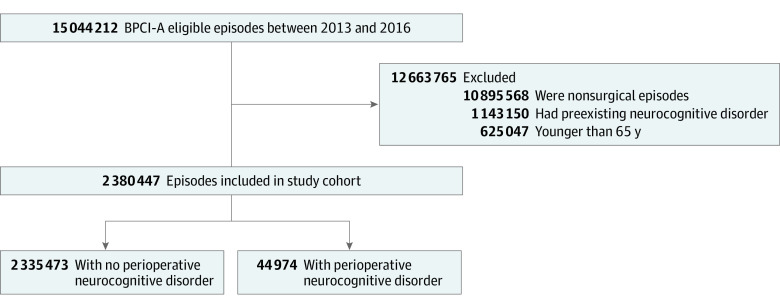
Design, setting, and participants: This retrospective cohort study used claims data from the Bundled Payments for Care Improvement Advanced Model from 4285 hospitals that submitted Medicare Fee-for-service (FFS) claims between January 2013 and December 2016. All Medicare patients aged 65 years or older who underwent an inpatient hospital admission associated with a surgical procedure, did not experience a PND before index admission, and were not undergoing dialysis or concurrently enrolled in Medicaid were included. Data were analyzed from October 2019 and May 2020.
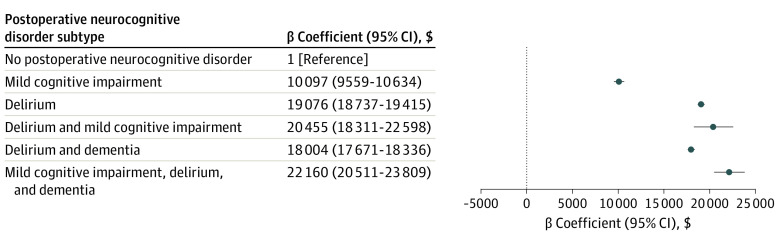
Exposures: PND, defined as an International Classification of Diseases, Ninth or Tenth Revision, diagnosis of delirium, mild cognitive impairment, or dementia within 1 year of discharge from the index surgical admission.
Main outcomes and measures: The primary outcome was total inflation-adjusted Medicare postacute care payments within 1 year after the index surgical procedure.
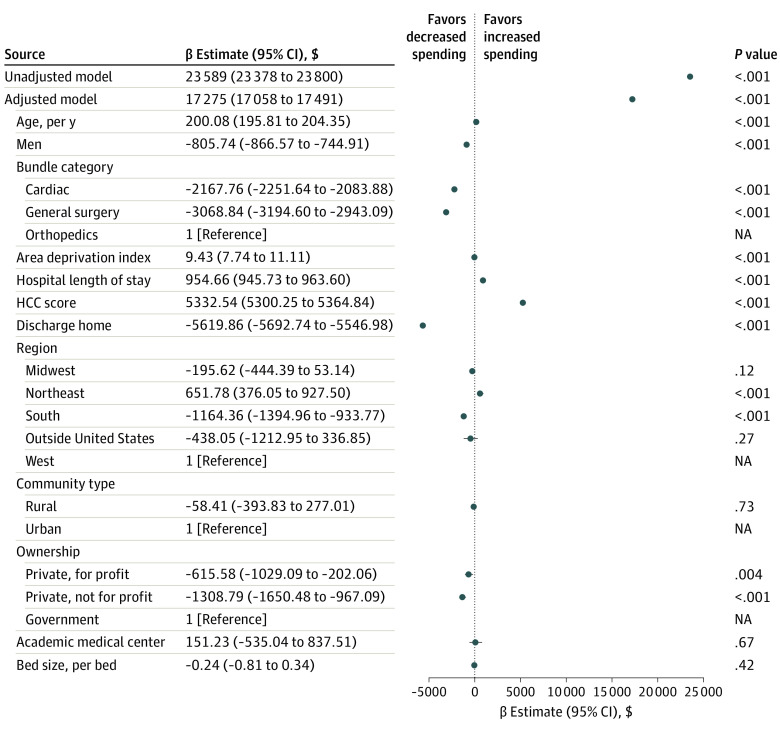
Results: A total of 2 380 473 patients (mean [SD] age, 75.36 (7.31) years; 1 336 736 [56.1%] women) who underwent surgical procedures were included, of whom 44 974 patients (1.9%) were diagnosed with a PND. Among all patients, most were White (2 142 157 patients [90.0%]), presenting for orthopedic surgery (1 523 782 patients [64.0%]) in urban medical centers (2 179 893 patients [91.6%]) that were private nonprofits (1 798 749 patients [75.6%]). Patients with a PND, compared with those without a PND, experienced a significantly longer hospital length of stay (mean [SD], 5.91 [6.01] days vs 4.29 [4.18] days; P < .001), were less likely to be discharged home (9947 patients [22.1%] vs 914 925 patients [39.2%]; P < .001), and had a higher incidence of mortality at 1 year after treatment (4580 patients [10.2%] vs 103 767 patients [4.4%]; P < .001). After adjusting for patient and hospital characteristics, the presence of a PND within 1 year of the index procedure was associated with an increase of $17 275 (95% CI, $17 058-$17 491) in cost in the 1-year postadmission period (P < .001).
Conclusions and relevance: The findings of this cohort study suggest that among older Medicare patients undergoing surgical treatment, a diagnosis of a PND was associated with an increase in health care costs for up to 1 year following the surgical procedure. Given the magnitude of this cost burden, PNDs represent an appealing target for risk mitigation and improvement in value-based health care.
Conflict of interest statement
Figures