

Machine learning reveals that Mycobacterium tuberculosis genotypes and anatomic disease site impacts drug resistance and disease transmission among patients with proven extra-pulmonary tuberculosis
- PMID: 32736602
- PMCID: PMC7393820
- DOI: 10.1186/s12879-020-05256-4
Machine learning reveals that Mycobacterium tuberculosis genotypes and anatomic disease site impacts drug resistance and disease transmission among patients with proven extra-pulmonary tuberculosis
Abstract
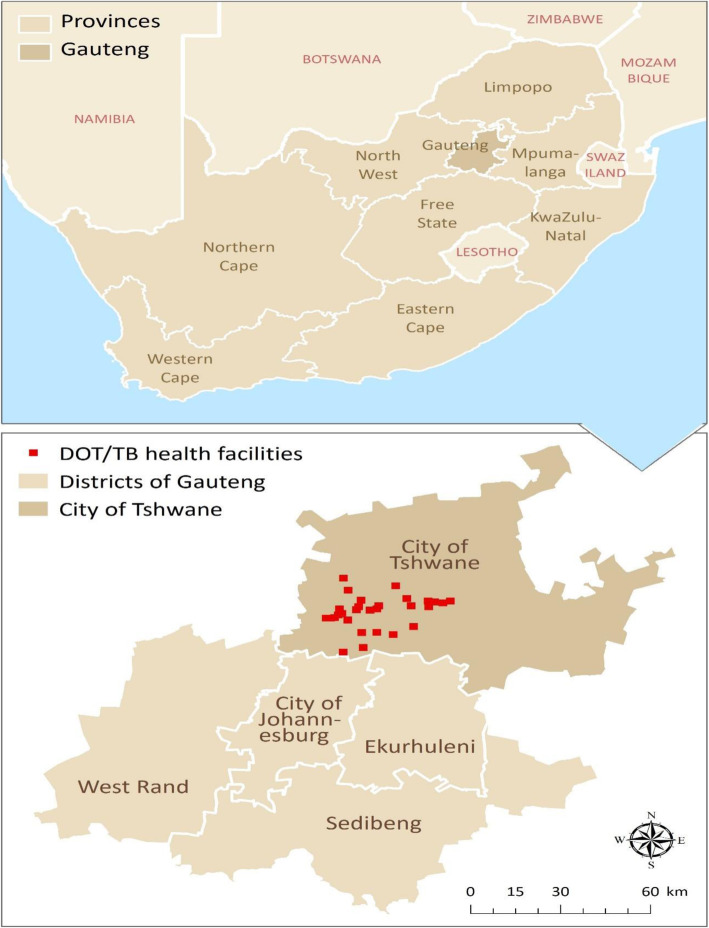
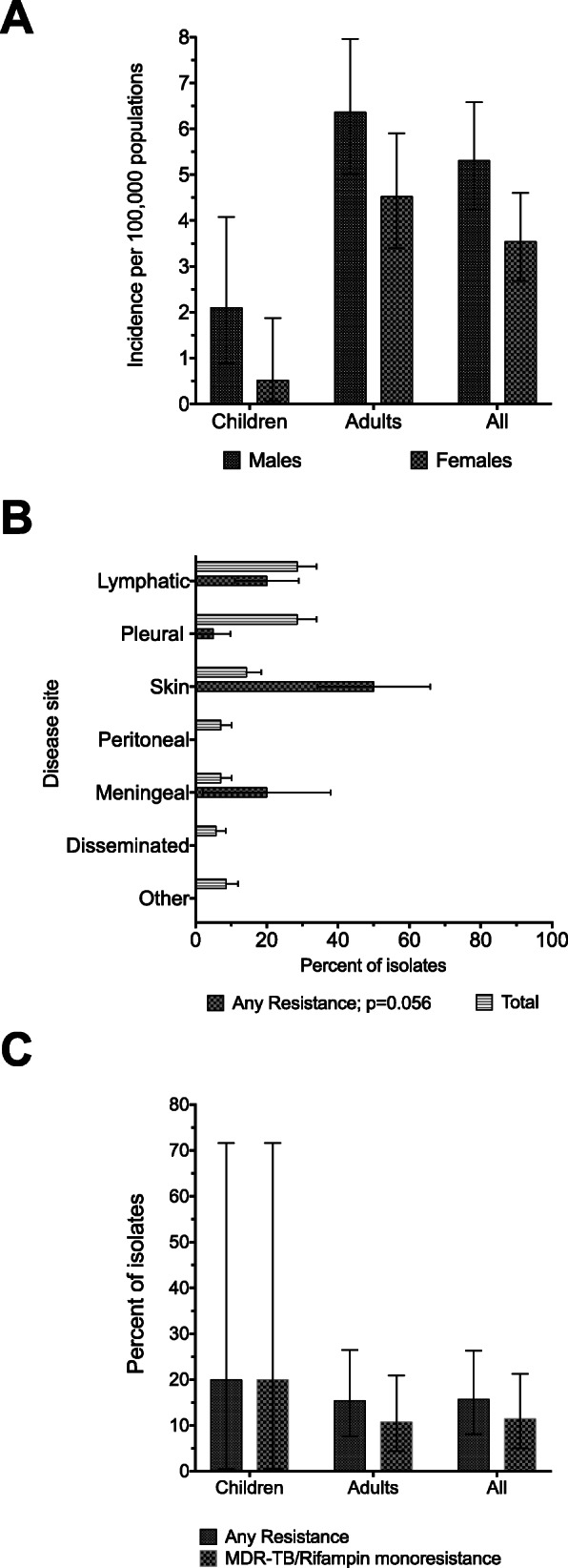
Background: There is a general dearth of information on extrapulmonary tuberculosis (EPTB). Here, we investigated Mycobacterium tuberculosis (Mtb) drug resistance and transmission patterns in EPTB patients treated in the Tshwane metropolitan area, in South Africa.
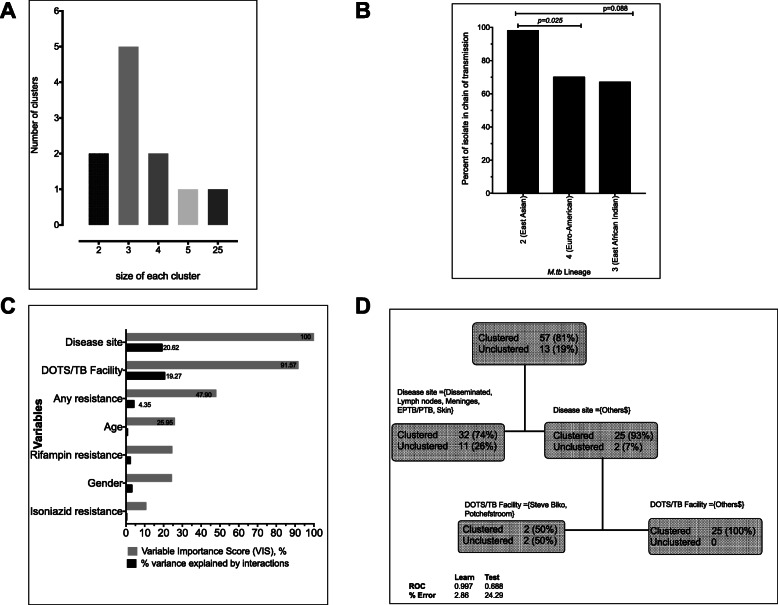
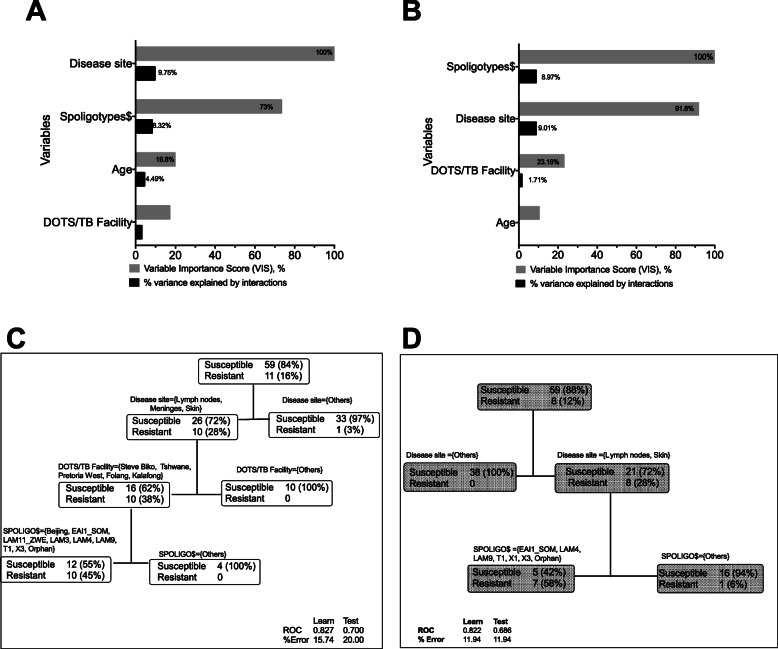
Methods: Consecutive Mtb culture-positive non-pulmonary samples from unique EPTB patients underwent mycobacterial genotyping and were assigned to phylogenetic lineages and transmission clusters based on spoligotypes. MTBDRplus assay was used to search mutations for isoniazid and rifampin resistance. Machine learning algorithms were used to identify clinically meaningful patterns in data. We computed odds ratio (OR), attributable risk (AR) and corresponding 95% confidence intervals (CI).
Results: Of the 70 isolates examined, the largest cluster comprised 25 (36%) Mtb strains that belonged to the East Asian lineage. East Asian lineage was significantly more likely to occur within chains of transmission when compared to the Euro-American and East-African Indian lineages: OR = 10.11 (95% CI: 1.56-116). Lymphadenitis, meningitis and cutaneous TB, were significantly more likely to be associated with drug resistance: OR = 12.69 (95% CI: 1.82-141.60) and AR = 0.25 (95% CI: 0.06-0.43) when compared with other EPTB sites, which suggests that poor rifampin penetration might be a contributing factor.
Conclusions: The majority of Mtb strains circulating in the Tshwane metropolis belongs to East Asian, Euro-American and East-African Indian lineages. Each of these are likely to be clustered, suggesting on-going EPTB transmission. Since 25% of the drug resistance was attributable to sanctuary EPTB sites notorious for poor rifampin penetration, we hypothesize that poor anti-tuberculosis drug dosing might have a role in the development of resistance.
Keywords: Acquired drug resistance; Attributable risk; Number needed to screen; Pharmacokinetic variability; Spoligotypes; Stochastic gradient boosting.
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
References
-
- Nanoo A, Izu A, Ismail NA, Ihekweazu C, Abubakar I, Mametja D, Madhi SA. Nationwide and regional incidence of microbiologically confirmed pulmonary tuberculosis in South Africa, 2004-12: a time series analysis. Lancet Infect Dis. 2015;15(9):1066–1076. - PubMed
-
- Dheda K, Gumbo T, Maartens G, Dooley KE, McNerney R, Murray M, Furin J, Nardell EA, London L, Lessem E, et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. 2017;5:291–360. - PubMed
-
- Marais BJ, Graham SM, Maeurer M, Zumla A. Progress and challenges in childhood tuberculosis. Lancet Infect Dis. 2013;13(4):287–289. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
