

doi: 10.1186/s13054-020-03176-y.
Development of a work of breathing scale and monitoring need of intubation in COVID-19 pneumonia
Affiliations
- PMID: 32736637
- PMCID: PMC7393620
- DOI: 10.1186/s13054-020-03176-y
Item in Clipboard
Development of a work of breathing scale and monitoring need of intubation in COVID-19 pneumonia
Crit Care.
.
No abstract available
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
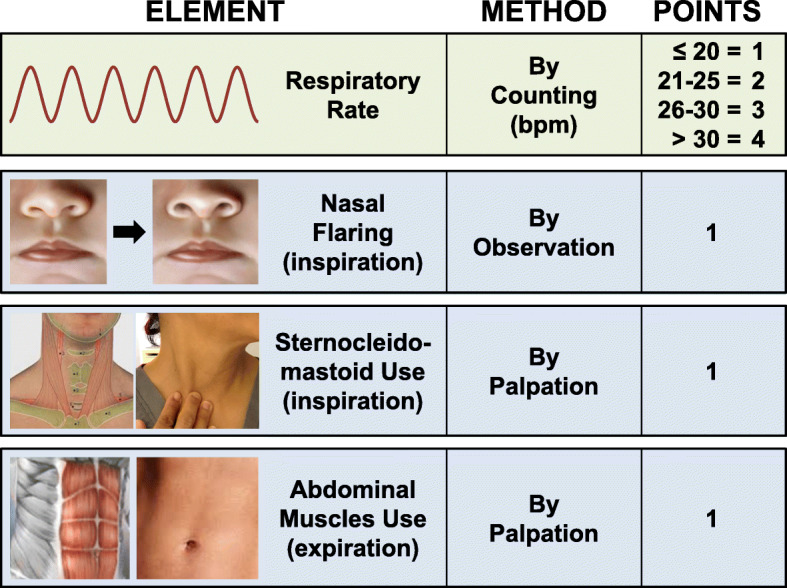
Work of breathing scale assigning points to the respiratory frequency and activation of respiratory accessory muscles. Nasal flaring is determined visually by noticing widening of the nostrils during inspiration while standing at approximately one-meter from the patient. Activation of the sternocleidomastoid is determined by gentle palpation of its clavicular insertion using two fingers from the hand ipsilateral to the patient’s side noticing increased tension during inspiration. Activation of abdominal muscles is determined by gentle palpation of the abdomen using the hand ipsilateral to the patient’s side noticing increased tension during expiration
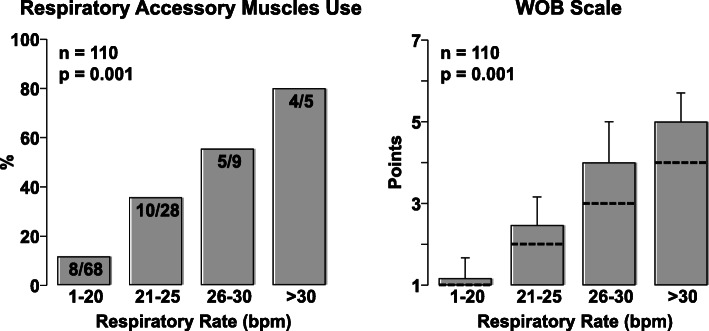
Left graph shows the percentage of patients who had activation of at least one of the accessory muscles assessed by the work breathing scale as a function of respiratory rate. Right graph shows the mean and standard deviation of the work breathing scale as a function of respiratory rate with the discontinuous line indicating the contribution of the respiratory rate alone (right). Analysis performed in 110 patients. Overall differences were analyzed using SigmaPlot 12.5 by chi-square on the left and by one-way analysis of variance on the right
References
-
- Marini JJ, Gattinoni L. Management of COVID-19 respiratory distress. JAMA. 2020;24:10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
