

The bone attachments of the medial collateral and posterior oblique ligaments are defined anatomically and radiographically
- PMID: 32737529
- PMCID: PMC7669814
- DOI: 10.1007/s00167-020-06139-6
The bone attachments of the medial collateral and posterior oblique ligaments are defined anatomically and radiographically
Abstract
Purpose: To define the bony attachments of the medial ligaments relative to anatomical and radiographic bony landmarks, providing information for medial collateral ligament (MCL) surgery.
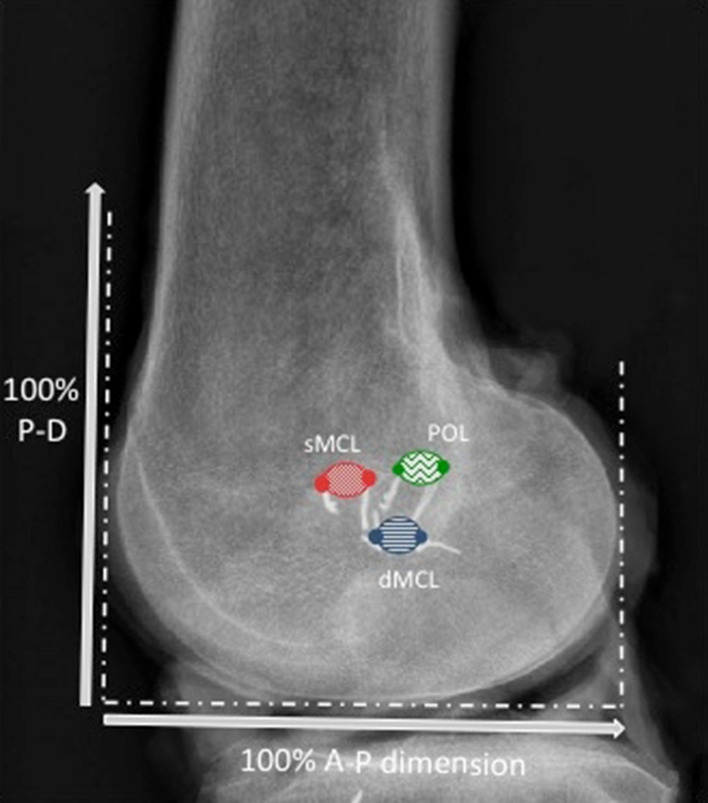
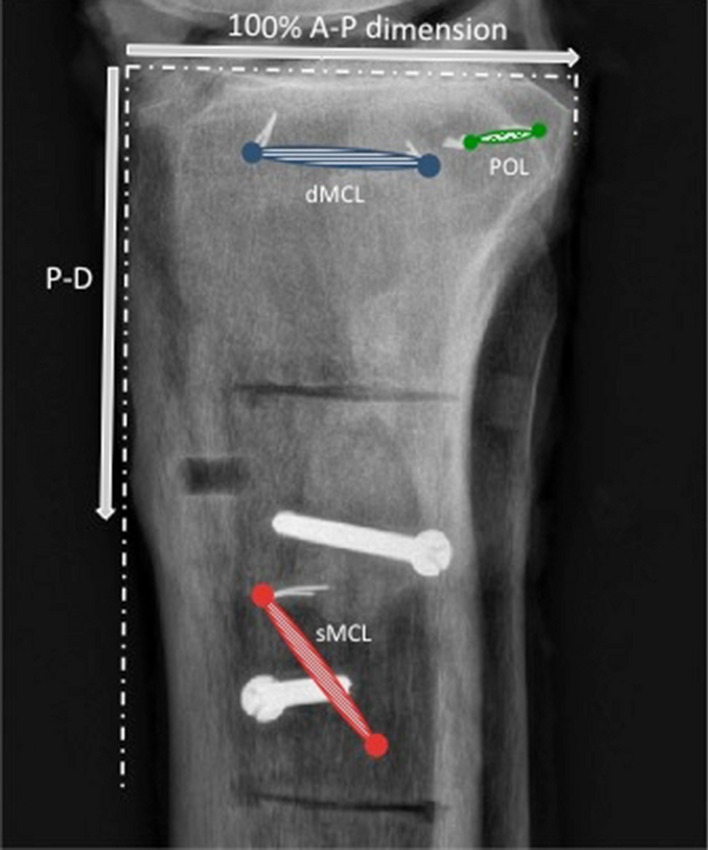
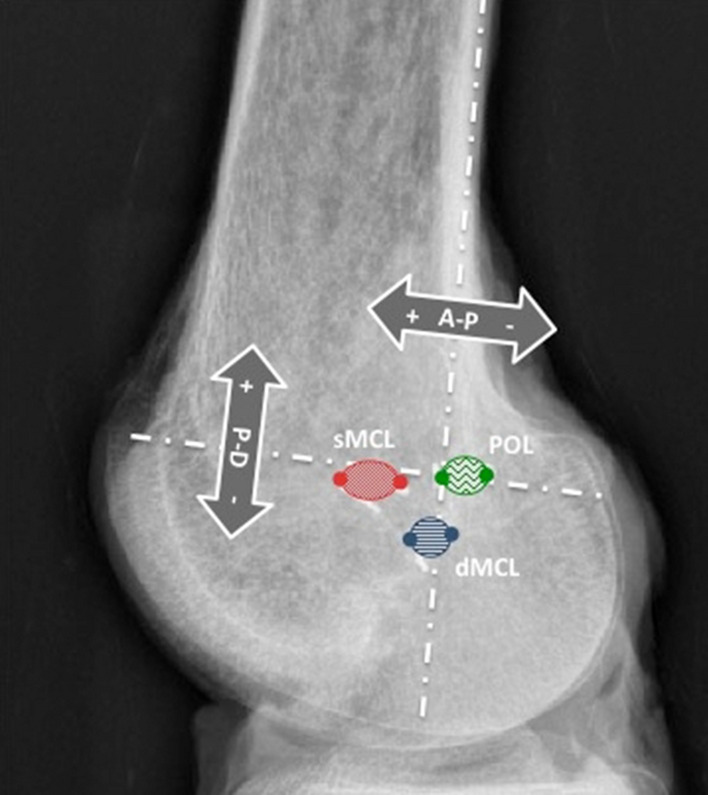
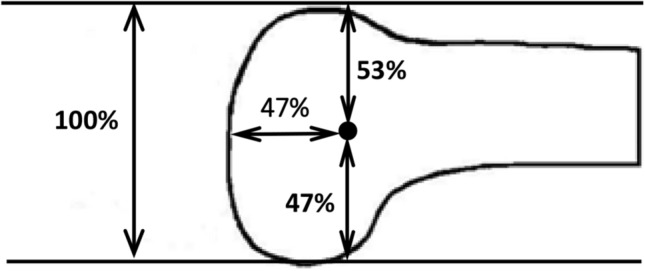
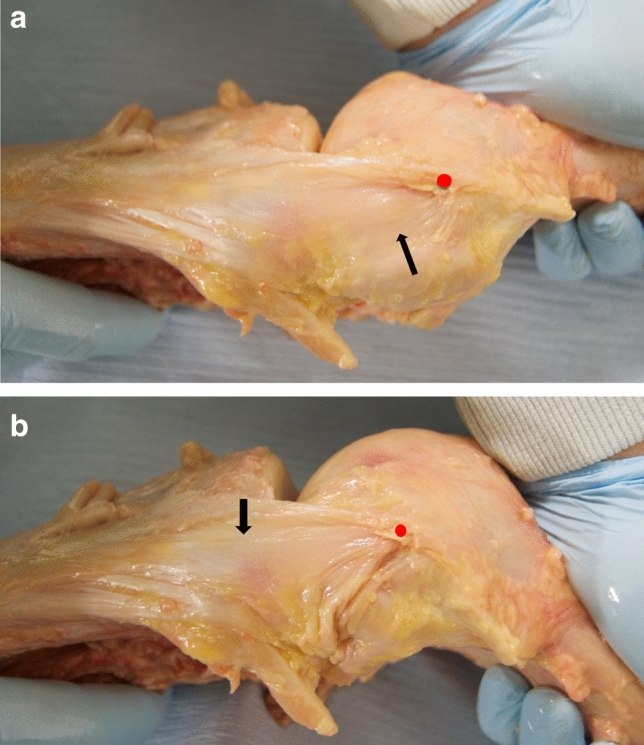
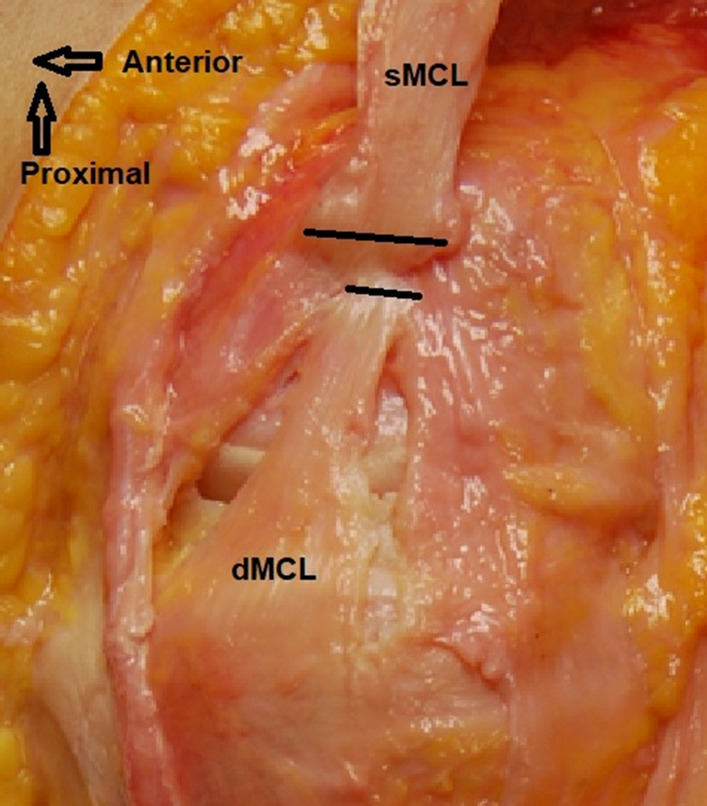
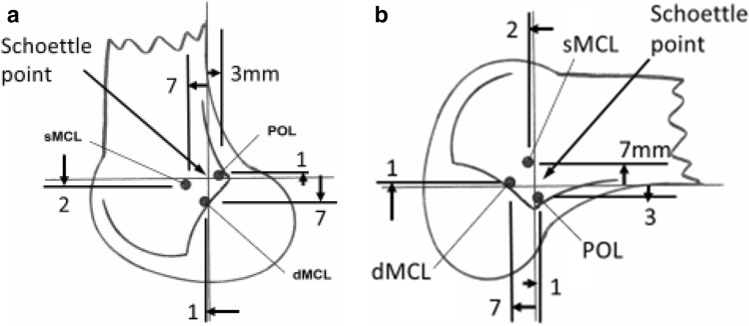
Method: The femoral and tibial attachments of the superficial MCL (sMCL), deep MCL (dMCL) and posterior oblique ligament (POL), plus the medial epicondyle (ME) were defined by radiopaque staples in 22 knees. These were measured radiographically and optically; the precision was calculated and data normalised to the sizes of the condyles. Femoral locations were referenced to the ME and to Blumensaat's line and the posterior cortex.
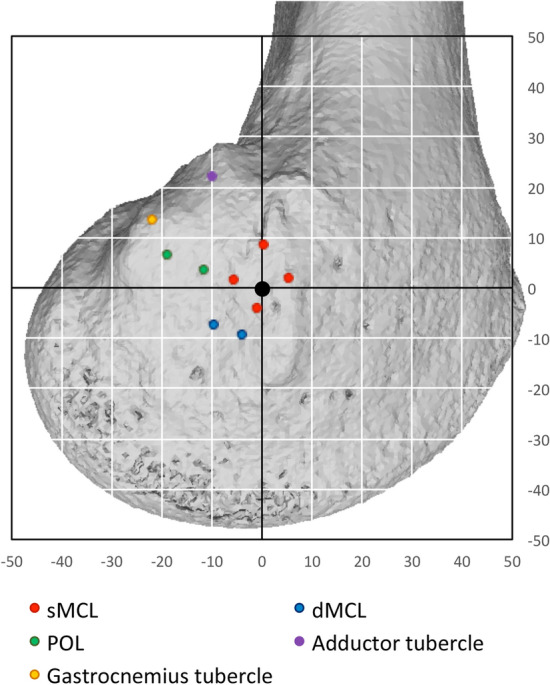
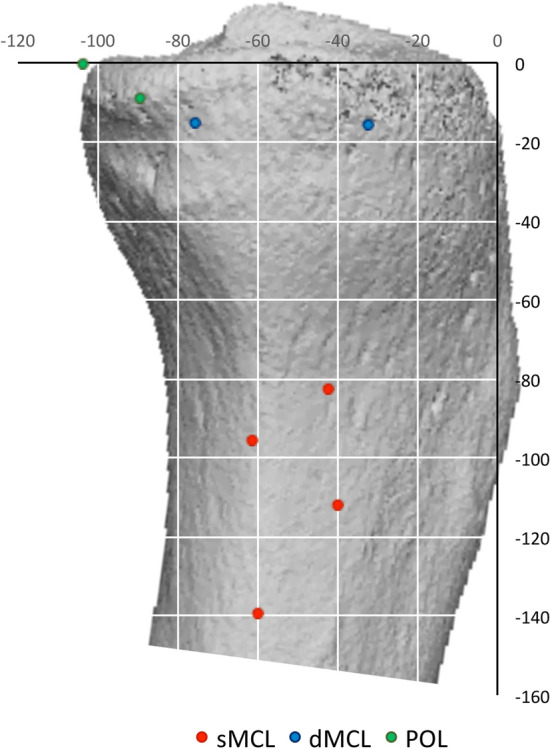
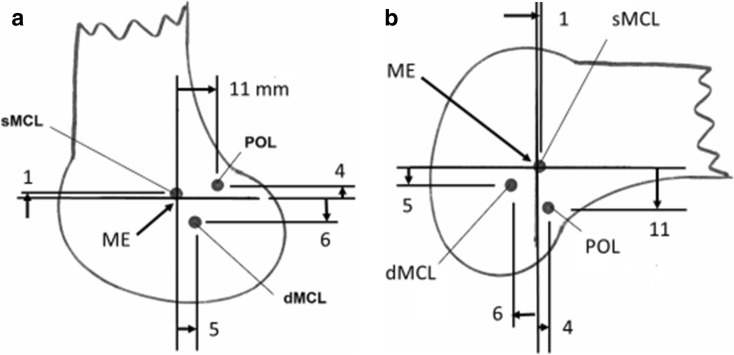
Results: The femoral sMCL attachment enveloped the ME, centred 1 mm proximal to it, at 37 ± 2 mm (normalised at 53 ± 2%) posterior to the most-anterior condyle border. The femoral dMCL attachment was 6 mm (8%) distal and 5 mm (7%) posterior to the ME. The femoral POL attachment was 4 mm (5%) proximal and 11 mm (15%) posterior to the ME. The tibial sMCL attachment spread from 42 to 71 mm (81-137% of A-P plateau width) below the tibial plateau. The dMCL fanned out anterodistally to a wide tibial attachment 8 mm below the plateau and between 17 and 39 mm (33-76%) A-P. The POL attached 5 mm below the plateau, posterior to the dMCL. The 95% CI intra-observer was ± 0.6 mm, inter-observer ± 1.3 mm for digitisation. The inter-observer ICC for radiographs was 0.922.
Conclusion: The bone attachments of the medial knee ligaments are located in relation to knee dimensions and osseous landmarks. These data facilitate repairs and reconstructions that can restore physiological laxity and stability patterns across the arc of knee flexion.
Keywords: Bone insertion attachment footprint; Knee anatomy; Medial collateral ligament; Posterior oblique ligament; Radiograph.
Conflict of interest statement
AAA: grant from Smith & Nephew Co, paid to a research account of Imperial College London; Paid speaker of Smith & Nephew Co. KKA: Supported by a grant from Smith & Nephew Co. SB: No conflicts of interest. SS: No conflicts of interest. AW: Director of Fortius Clinic; Director of Innovation Orthopaedics; Paid speaker of Smith & Nephew Co. LW: Supported by a grant from the German Research Foundation DFG.
Figures
References
-
- Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. 1994;6(4):284–290. doi: 10.1037/1040-3590.6.4.284. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
