

Prenatal Exposure to Perfluoroalkyl Substances Associated With Increased Susceptibility to Liver Injury in Children
- PMID: 32738061
- PMCID: PMC7723317
- DOI: 10.1002/hep.31483
Prenatal Exposure to Perfluoroalkyl Substances Associated With Increased Susceptibility to Liver Injury in Children
Abstract
Background and aims: Per- and polyfluoroalkyl substances (PFAS) are widespread and persistent pollutants that have been shown to have hepatotoxic effects in animal models. However, human evidence is scarce. We evaluated how prenatal exposure to PFAS associates with established serum biomarkers of liver injury and alterations in serum metabolome in children.
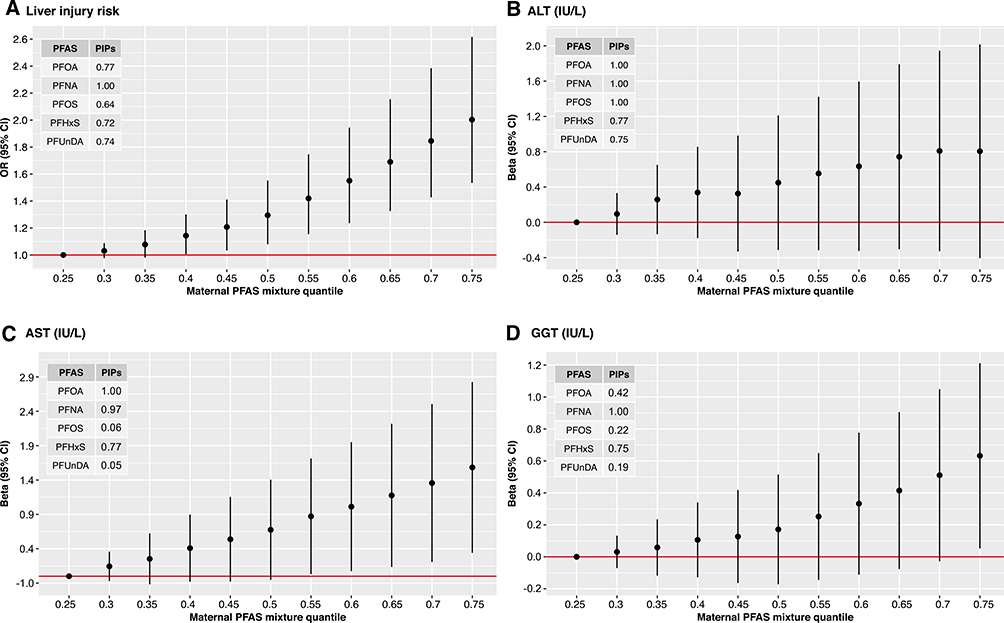
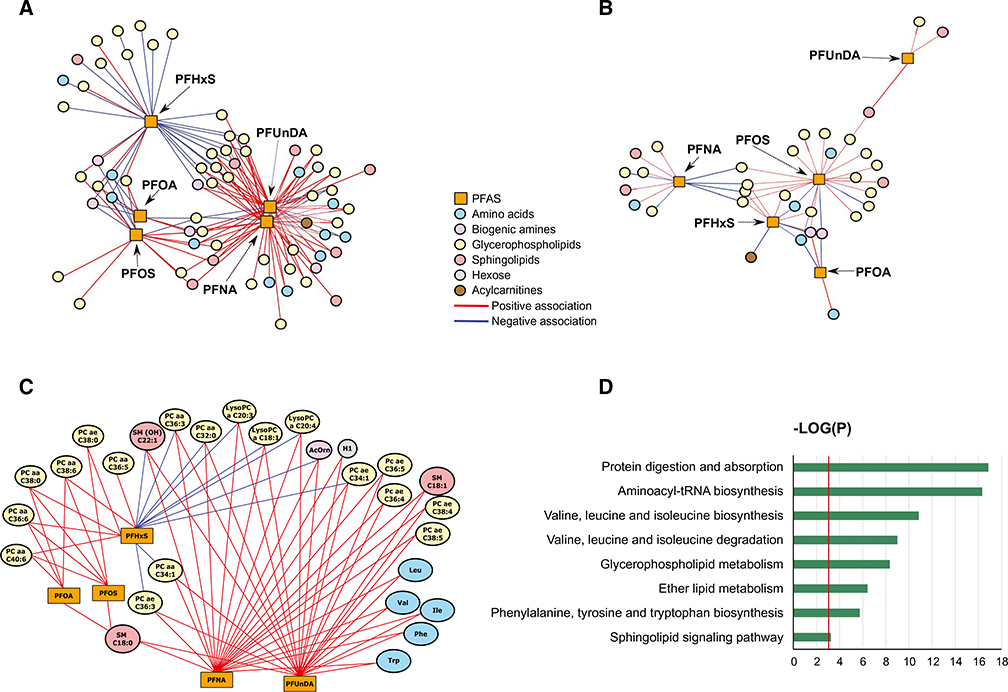
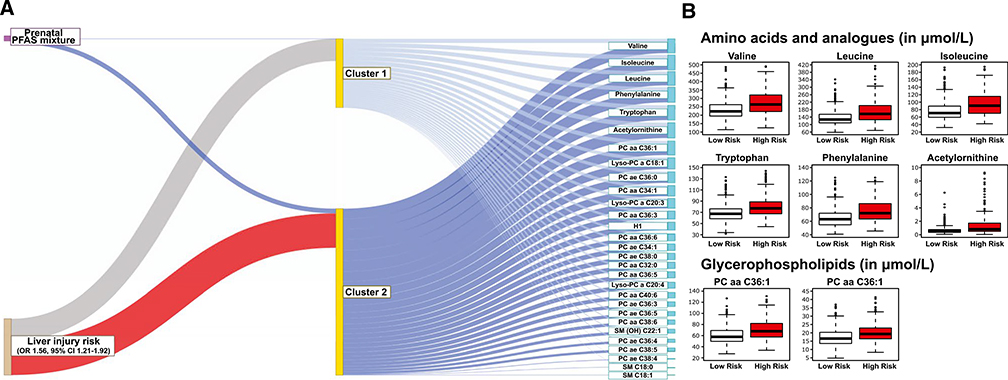
Approach and results: We used data from 1,105 mothers and their children (median age, 8.2 years; interquartile range, 6.6-9.1) from the European Human Early-Life Exposome cohort (consisting of six existing population-based birth cohorts in France, Greece, Lithuania, Norway, Spain, and the United Kingdom). We measured concentrations of perfluorooctane sulfonate, perfluorooctanoate, perfluorononanoate, perfluorohexane sulfonate, and perfluoroundecanoate in maternal blood. We assessed concentrations of alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyltransferase in child serum. Using Bayesian kernel machine regression, we found that higher exposure to PFAS during pregnancy was associated with higher liver enzyme levels in children. We also measured child serum metabolomics through a targeted assay and found significant perturbations in amino acid and glycerophospholipid metabolism associated with prenatal PFAS. A latent variable analysis identified a profile of children at high risk of liver injury (odds ratio, 1.56; 95% confidence interval, 1.21-1.92) that was characterized by high prenatal exposure to PFAS and increased serum levels of branched-chain amino acids (valine, leucine, and isoleucine), aromatic amino acids (tryptophan and phenylalanine), and glycerophospholipids (phosphatidylcholine [PC] aa C36:1 and Lyso-PC a C18:1).
Conclusions: Developmental exposure to PFAS can contribute to pediatric liver injury.
© 2020 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: Nothing to report.
Figures
Comment in
-
Environmental Pollution and the Developmental Origins of Childhood Liver Disease.Hepatology. 2020 Nov;72(5):1518-1521. doi: 10.1002/hep.31549. Hepatology. 2020. PMID: 32910501 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- R21 ES029681/ES/NIEHS NIH HHS/United States
- P01 ES022845/ES/NIEHS NIH HHS/United States
- MR/N024397/1/MRC_/Medical Research Council/United Kingdom
- R01 ES030691/ES/NIEHS NIH HHS/United States
- R01 CA140561/CA/NCI NIH HHS/United States
- F32 ES029828/ES/NIEHS NIH HHS/United States
- R01 ES030364/ES/NIEHS NIH HHS/United States
- P30 DK048522/DK/NIDDK NIH HHS/United States
- P01 CA196569/CA/NCI NIH HHS/United States
- R01 ES029944/ES/NIEHS NIH HHS/United States
- P30 ES007048/ES/NIEHS NIH HHS/United States
- R21 ES028903/ES/NIEHS NIH HHS/United States
- R21ES029681/ES/NIEHS NIH HHS/United States
- R01 ES016813/ES/NIEHS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
