

Trauma of major surgery: A global problem that is not going away
- PMID: 32738546
- PMCID: PMC7388795
- DOI: 10.1016/j.ijsu.2020.07.017
Trauma of major surgery: A global problem that is not going away
Abstract
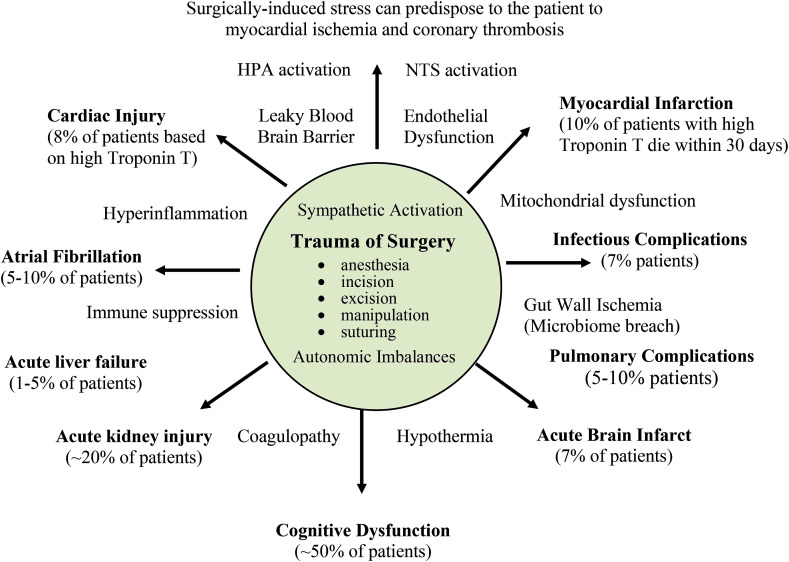
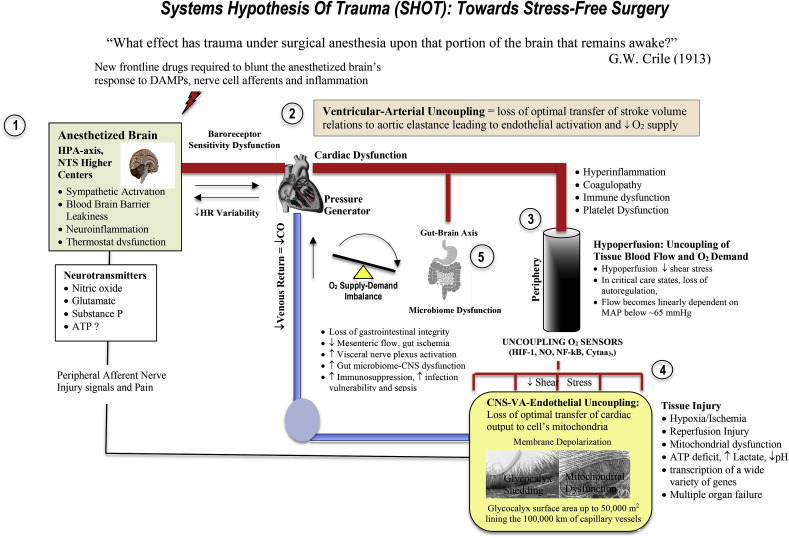
Globally, a staggering 310 million major surgeries are performed each year; around 40 to 50 million in USA and 20 million in Europe. It is estimated that 1-4% of these patients will die, up to 15% will have serious postoperative morbidity, and 5-15% will be readmitted within 30 days. An annual global mortality of around 8 million patients places major surgery comparable with the leading causes of death from cardiovascular disease and stroke, cancer and injury. If surgical complications were classified as a pandemic, like HIV/AIDS or coronavirus (COVID-19), developed countries would work together and devise an immediate action plan and allocate resources to address it. Seeking to reduce preventable deaths and post-surgical complications would save billions of dollars in healthcare costs. Part of the global problem resides in differences in institutional practice patterns in high- and low-income countries, and part from a lack of effective perioperative drug therapies to protect the patient from surgical stress. We briefly review the history of surgical stress and provide a path forward from a systems-based approach. Key to progress is recognizing that the anesthetized brain is still physiologically 'awake' and responsive to the sterile stressors of surgery. New intravenous drug therapies are urgently required after anesthesia and before the first incision to prevent the brain from switching to sympathetic overdrive and activating secondary injury progression such as hyperinflammation, coagulopathy, immune activation and metabolic dysfunction. A systems-based approach targeting central nervous system-mitochondrial coupling may help drive research to improve outcomes following major surgery in civilian and military medicine.
Keywords: Global; Morbidity; Mortality; Perioperative; Surgery; Trauma.
Copyright © 2020 IJS Publishing Group Ltd. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Geoffrey Dobson is the sole inventor of the ALM concept for cardioplegia, organ preservation, surgery, infection and trauma, and has no financial interests from any entity or organization.
Figures
References
-
- Weiser T.G., Regenbogen S.E., Thompson K.D., Haynes A.B., Lipsitz S.R., Berry W.R., Gawande A.A. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372(9633):139–144. - PubMed
-
- Weiser T.G., Haynes A.B., Molina G., Lipsitz S.R., Esquivel M.M., Uribe-Leitz T., Fu R., Azad T., Chao T.E., Berry W.R., et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015:385. - PubMed
-
- Maggio P.M., Taheri P.A. Perioperative issues: myocardial ischemia and protection--beta-blockade. Surg. Clin. 2005;85(6):1091–1102. - PubMed
-
- Patel A.Y., Eagle K.A. Cardiac risk of noncardiac surgery. J. Am. Coll. Cardiol. 2015;66(19):2140–2148. - PubMed
-
- Kristensen S.D., Knuuti J., Saraste A., Anker S., Bøtker H.E., Hert S.D., Ford I., Gonzalez-Juanatey J.R., Gorenek B., Heyndrickx G.R., et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management. Eur. Heart J. 2014;35:2383–2431. Sept 14 (35) - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical