

Comment
doi: 10.1016/j.jpeds.2020.07.079.
Epub 2020 Jul 30.
Management of Post-hemorrhagic Ventricular Dilatation in the Infant Born Preterm
Affiliations
- PMID: 32739263
- PMCID: PMC8297821
- DOI: 10.1016/j.jpeds.2020.07.079
Item in Clipboard
Comment
Management of Post-hemorrhagic Ventricular Dilatation in the Infant Born Preterm
J Pediatr.
2020 Nov.
No abstract available
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
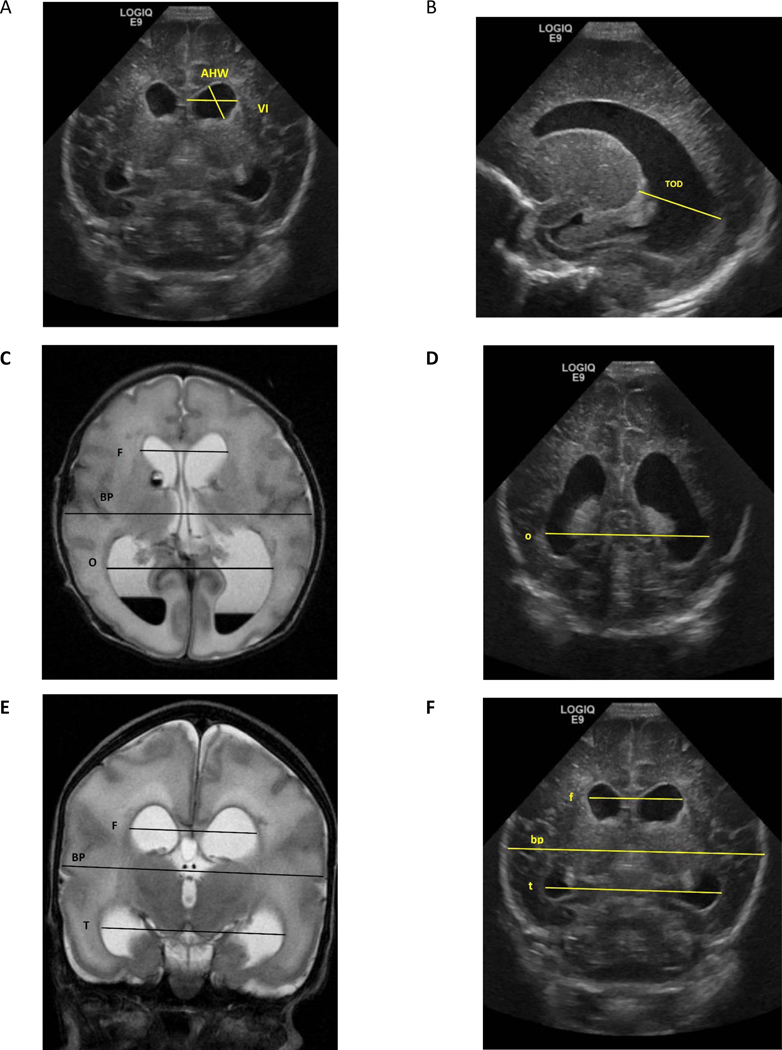
Images from cUS and brain MRI of one-week old boy born at 30 weeks of gestation. A and F= Coronal cUS at level of Foramen of Monro, B= Parasagittal cUS, C= Axial View of T2 MRI. D= Coronal cUS at level of occipital horn E= Coronal View of T2 MRI, VI= Ventricular Index, AHW= Anterior Horn Width, TOD= Thalamo-Occipital Diameter MRI dimensions are in Capital letters= F= bifrontal horn, BP= biparietal, T= bitemporal horn, O =bioccipital horn cUS dimensions are in small letters= f= bifrontal horn, bp= biparietal, t= bitemporal horn, o =bioccipital horn Evans Ratio= F/BP by MRI or f/bp by US Frontal and Temporal Horn Ratio= (F+T/2)/ BP by MRI or (f+t/2)/bp by cUS Frontal and Occipital Horn Ratio (FOHR)= (F+O/2)/BP by MRI or (f+o/2)/bp by cUS
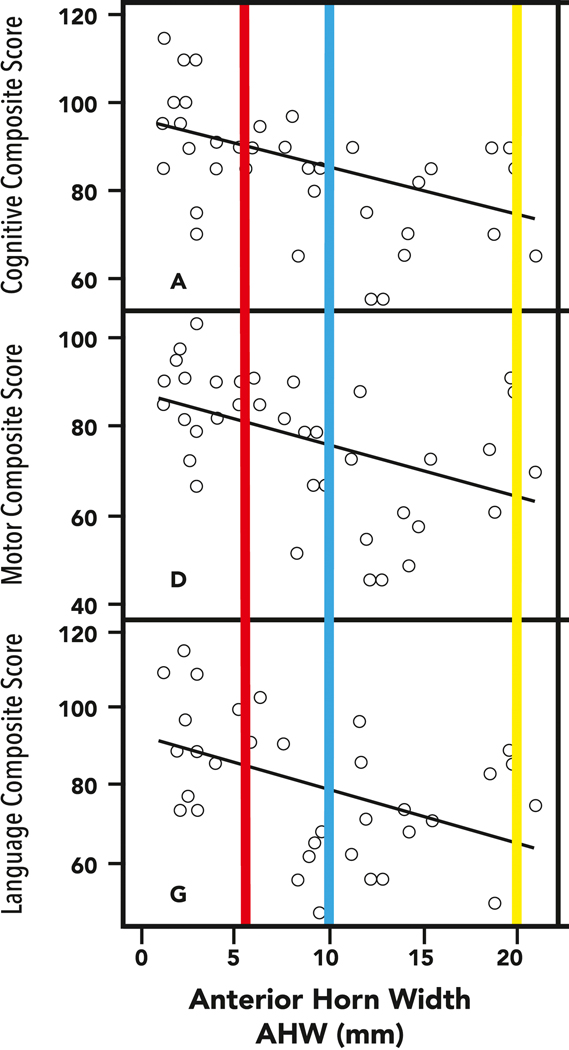
Anterior Horn Width in relation to neurodevelopmental outcomes at 18–24 months in 39 preterm infants with PHVD. The maximal size of the AHW in the North American group of the study by Leijser et al, (yellow bar) and the corresponding neurodevelopmental impairments with performance at 60–70 points, contrasts with the results in the ELVIS study with early (red) and late (blue) demonstrating less significant differences in outcomes. It is noteworthy that timing of the “late” intervention arm in ELVIS is much earlier than in the North American sites.
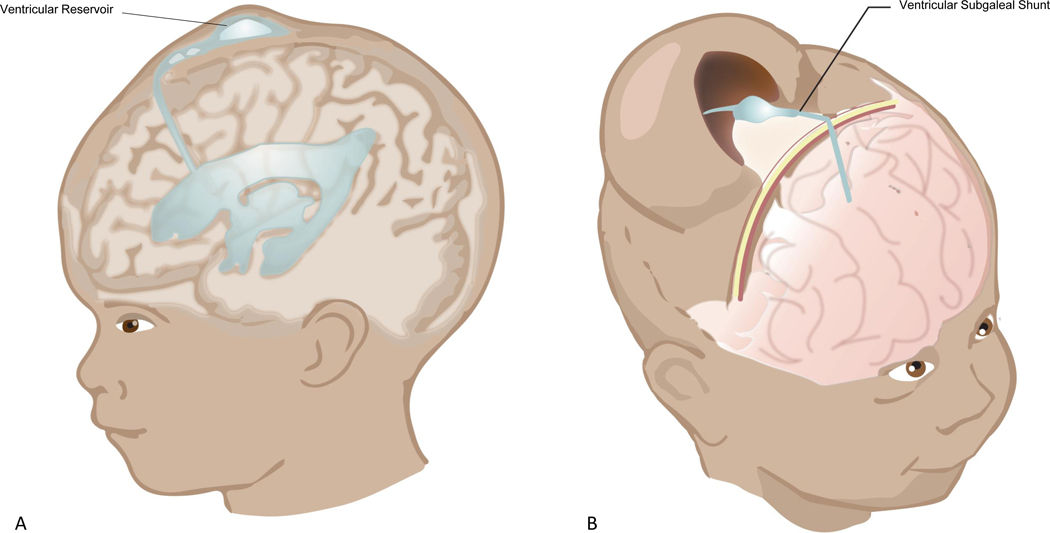
online: An illustration of the commonly used temporizing measures for PHVD: A) Ventricular Reservoir (VR), and B) Ventricular Subgaleal Shunt (VSGS)
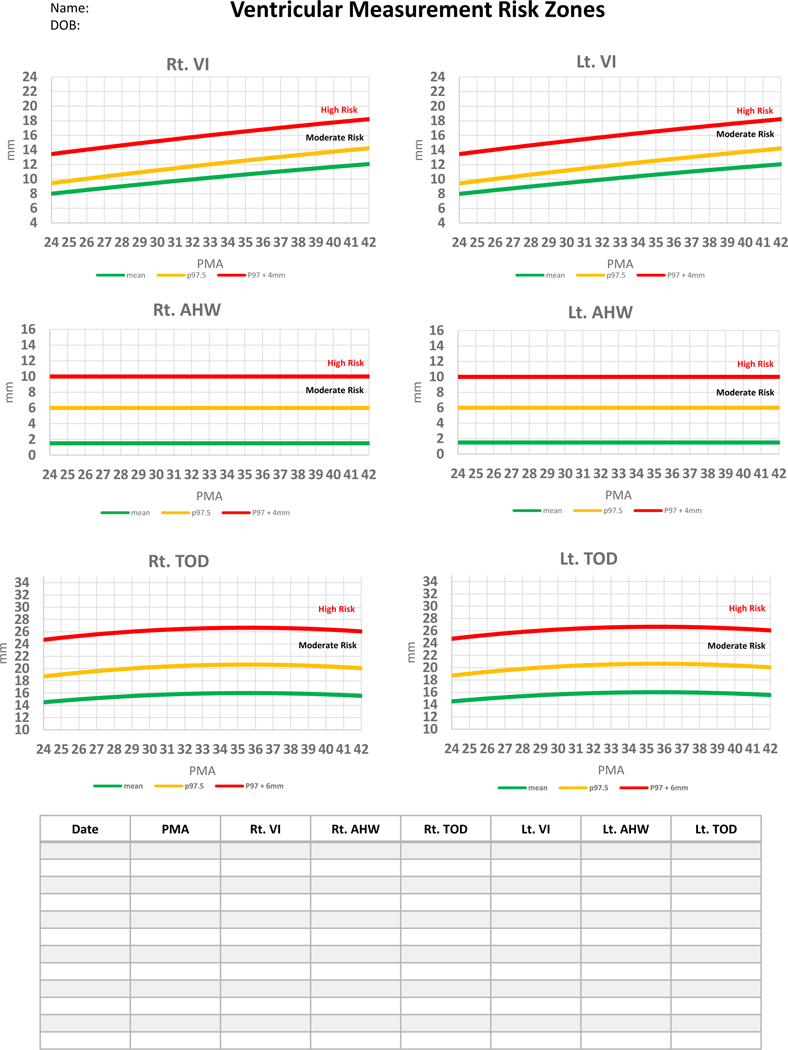
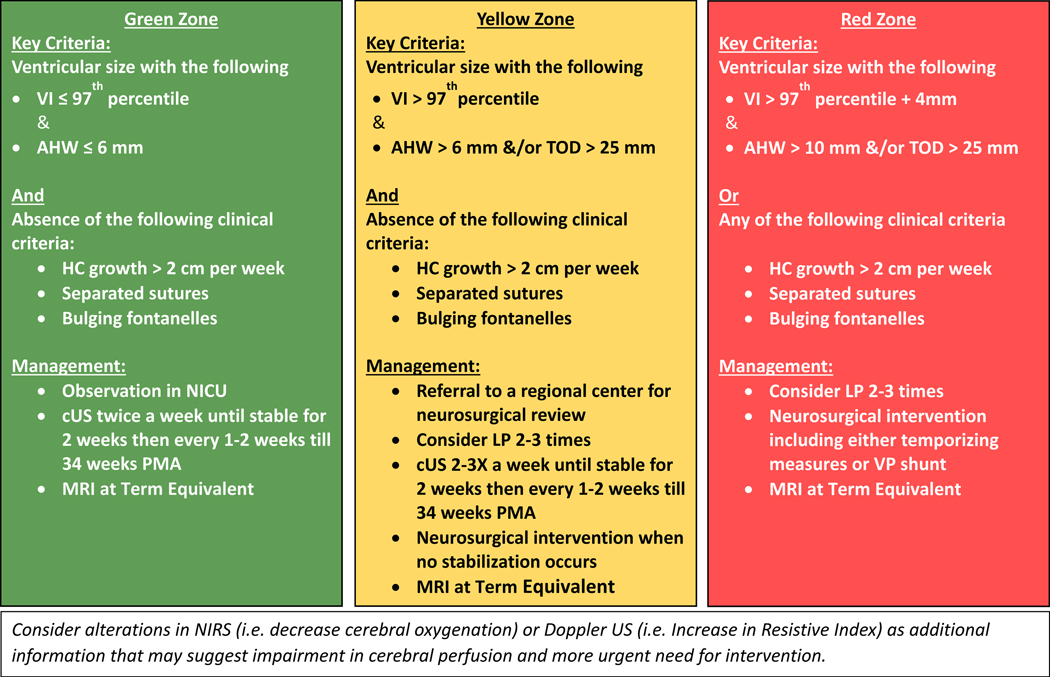
Individual measures can be plotted in mm in the table as well as on the corresponding postmenstrual age in the graph to identify risk zone. VI= Ventricular Index, AHW= Anterior Horn Width, TOD= Thalamo-Occipital Diameter
Comment on
-
Outcomes Following Post-Hemorrhagic Ventricular Dilatation among Infants of Extremely Low Gestational Age.J Pediatr. 2020 Nov;226:36-44.e3. doi: 10.1016/j.jpeds.2020.07.080. Epub 2020 Jul 30. J Pediatr. 2020. PMID: 32739261 Free PMC article.
-
Randomized Controlled Early versus Late Ventricular Intervention Study in Posthemorrhagic Ventricular Dilatation: Outcome at 2 Years.J Pediatr. 2020 Nov;226:28-35.e3. doi: 10.1016/j.jpeds.2020.08.014. Epub 2020 Aug 12. J Pediatr. 2020. PMID: 32800815 Clinical Trial.
References
-
- Kinney HC, Volpe JJ. Organizational events In: Volpe JJ, Inder TE, Darras BT, deVries LS, duPlessis AJ, Neil JJ, et al., editors. Volpe’s Neurology of the Newborn. Chapter 7, 6th ed. Philadelphia, PA: Elsevier; 2018. p. 145–75.
-
- Volpe JJ. Dysmaturation of premature brain: Importance, cellular mechanisms and potential interventions. Pediatr Neurol. 2019;95:42–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
