

Association of Implementation and Social Network Factors With Patient Safety Culture in Medical Homes: A Coincidence Analysis
- PMID: 32740134
- PMCID: PMC7855411
- DOI: 10.1097/PTS.0000000000000752
Association of Implementation and Social Network Factors With Patient Safety Culture in Medical Homes: A Coincidence Analysis
Abstract
Objectives: The patient-centered medical home (PCMH) may provide a key model for ambulatory patient safety. Our objective was to explore which PCMH and patient safety implementation and social network factors may be necessary or sufficient for higher patient safety culture.
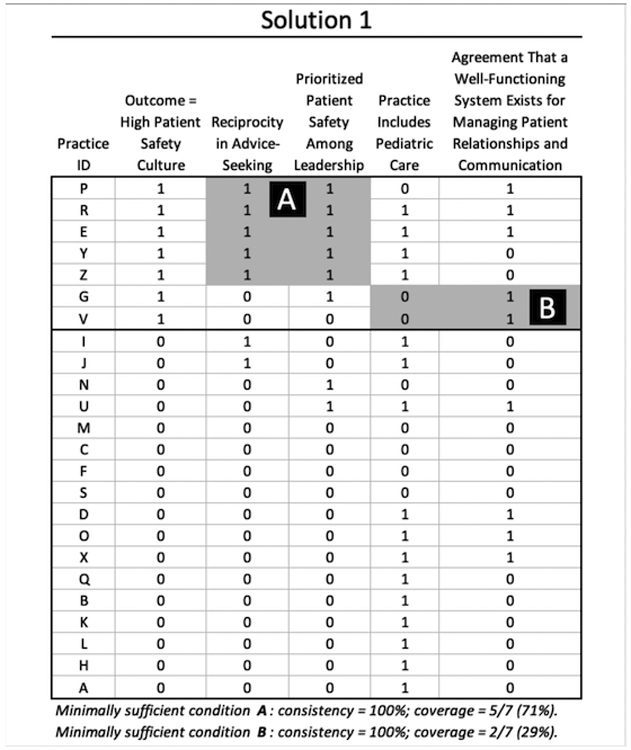
Methods: This was a cross-case analysis study in 25 diverse U.S. PCMHs. Data sources included interviews of a clinician and an administrator in each PCMH, surveys of clinicians and staff, and existing data on the PCMHs' characteristics. We used coincidence analysis, a novel method based on set theory and Boolean logic, to evaluate relationships between factors and the implementation outcome of patient safety culture.
Results: The coincidence analysis identified 5 equally parsimonious solutions (4 factors), accounting for all practices with higher safety culture. Three solutions contained the same core minimally sufficient condition: the implementation factor leadership priority for patient safety and the social network factor reciprocity in advice-seeking network ties (advice-seeking relationships). This minimally sufficient condition had the highest coverage (5/7 practices scoring higher on the outcome) and best performance across solutions; all included leadership priority for patient safety. Other key factors included self-efficacy and job satisfaction and quality improvement climate. The most common factor whose absence was associated with the outcome was a well-functioning process for behavioral health.
Conclusions: Our findings suggest that PCMH safety culture is higher when clinicians and staff perceive that leadership prioritizes patient safety and when high reciprocity among staff exists. Interventions to improve patient safety should consider measuring and addressing these key factors.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflict of interest. This research was funded by the Agency for Healthcare Research and Quality (grant number R01 HS024859). The views expressed are those of the authors and not necessarily those of the Agency for Healthcare Research and Quality.
Figures

References
-
- Joint Commission. 2019 National Patient Safety Goals. 2019; https://www.jointcommission.org/standards_information/npsgs.aspx. Accessed August 14th, 2019.
-
- American College of Physicians. Patient Safety in the Office-Based Practice Setting. Philadelphia, PA: American College of Physicians; 2017. Available at: https://www.acponline.org/acp_policy/policies/patient_safety_in_the_offi.... Accessed on August 28th, 2019.
-
- Shekelle PG, Sarkar U, Shojania K, et al. AHRQ Comparative Effectiveness Technical Briefs. In: Patient Safety in Ambulatory Settings. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016. - PubMed
-
- Webster JS, King HB, Toomey LM, et al. Understanding Quality and Safety Problems in the Ambulatory Environment: Seeking Improvement With Promising Teamwork Tools and Strategies. In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 3: Performance and Tools). Rockville (MD): Agency for Healthcare Research and Quality (US); 2008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
