

Validation of International Classification of Diseases, Tenth Revision, Clinical Modification Codes for Identifying Cases of Chlamydia and Gonorrhea
- PMID: 32740450
- PMCID: PMC7855200
- DOI: 10.1097/OLQ.0000000000001257
Validation of International Classification of Diseases, Tenth Revision, Clinical Modification Codes for Identifying Cases of Chlamydia and Gonorrhea
Abstract
Background: While researchers seek to use administrative health data to examine outcomes for individuals with sexually transmitted infections (STIs), the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes used to identify persons with chlamydia and gonorrhea have not been validated. Objectives were to determine the validity of using ICD-10-CM codes to identify individuals with chlamydia and gonorrhea.
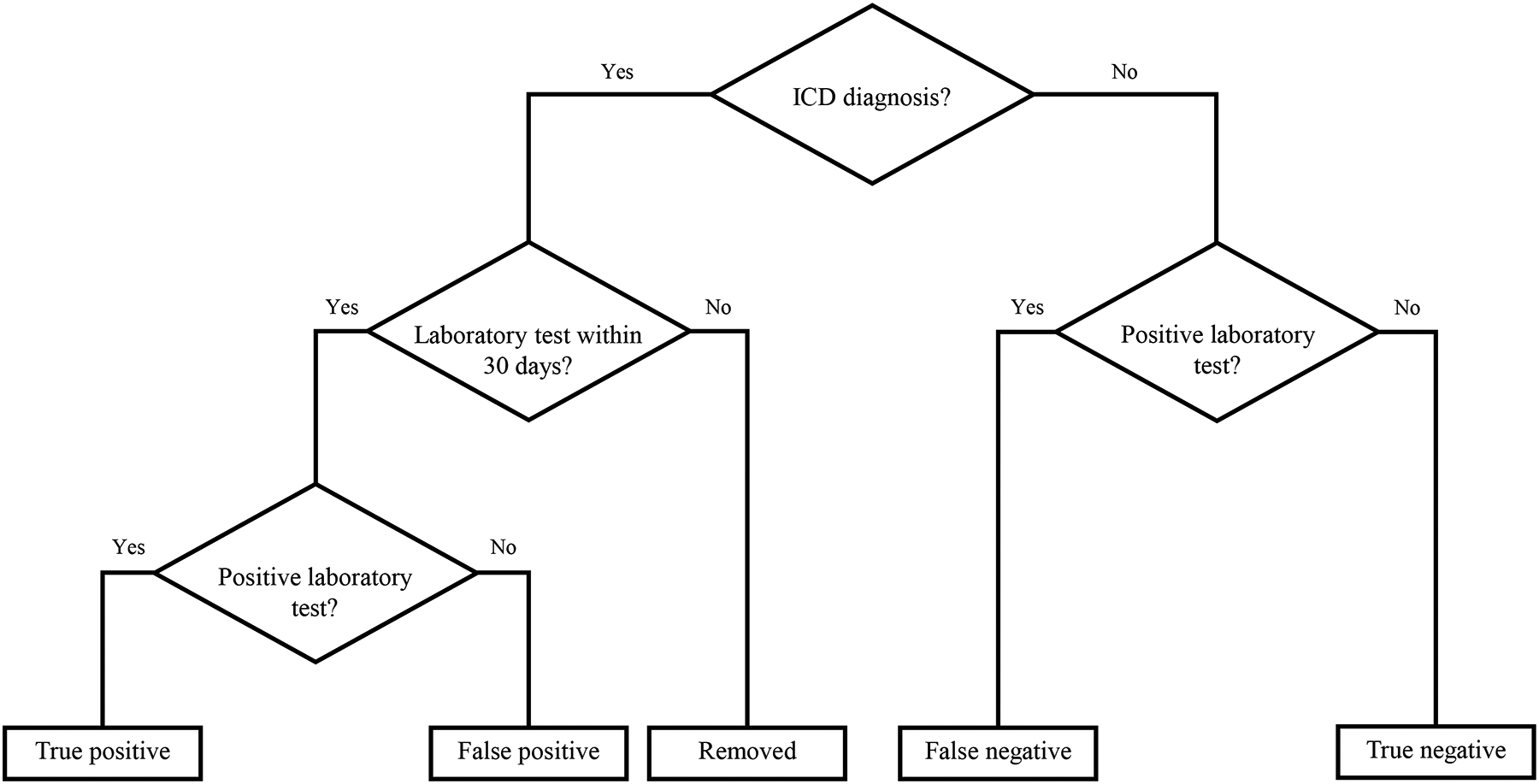
Methods: We used data from electronic health records gathered from public and private health systems from October 1, 2015, to December 31, 2016. Patients were included if they were aged 13 to 44 years and received either (1) laboratory testing for chlamydia or gonorrhea or (2) an ICD-10-CM diagnosis of chlamydia, gonorrhea, or an unspecified STI. To validate ICD-10-CM codes, we calculated positive and negative predictive values, sensitivity, and specificity based on the presence of a laboratory test result. We further examined the timing of clinical diagnosis relative to laboratory testing.
Results: The positive predictive values for chlamydia, gonorrhea, and unspecified STI ICD-10-CM codes were 87.6%, 85.0%, and 32.0%, respectively. Negative predictive values were high (>92%). Sensitivity for chlamydia diagnostic codes was 10.6%, and gonorrhea was 9.7%. Specificity was 99.9% for both chlamydia and gonorrhea. The date of diagnosis occurred on or after the date of the laboratory result for 84.8% of persons with chlamydia, 91.9% for gonorrhea, and 23.5% for unspecified STI.
Conclusions: Disease-specific ICD-10-CM codes accurately identify persons with chlamydia and gonorrhea. However, low sensitivities suggest that most individuals could not be identified in administrative data alone without laboratory test results.
Copyright © 2020 American Sexually Transmitted Diseases Association. All rights reserved.
Conflict of interest statement
Conflict of Interest and Sources of Funding: The authors report no conflicts of interest. This work was supported by a contract from the US Centers for Disease Control and Prevention (contract number: 2017-Q-67119) and a grant from the US National Library of Medicine (grant number: T15LM012502). The views expressed in this publication are those of the authors and do not necessarily reflect the position or policy of the Centers for Disease Control and Prevention, National Library of Medicine, or the US government.
Figures

References
-
- Iezzoni LI. Assessing Quality Using Administrative Data. Ann Intern Med. 1997;127(8_Part_2):666–674. - PubMed
-
- Kerr EA, McGlynn EA, Van Vorst KA, Wickstrom SL. Measuring Antidepressant Prescribing Practice in a Health Care System Using Administrative Data: Implications for Quality Measurement and Improvement. The Joint Commission Journal on Quality Improvement. 2000;26(4):203–216. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
