

Evaluation of Antibiotic Utilization in an Emergency Department After Implementation of an Antimicrobial Stewardship Pharmacist Culture Review Service
- PMID: 32742015
- PMCID: PMC7370348
- DOI: 10.1177/0018578719844171
Evaluation of Antibiotic Utilization in an Emergency Department After Implementation of an Antimicrobial Stewardship Pharmacist Culture Review Service
Abstract
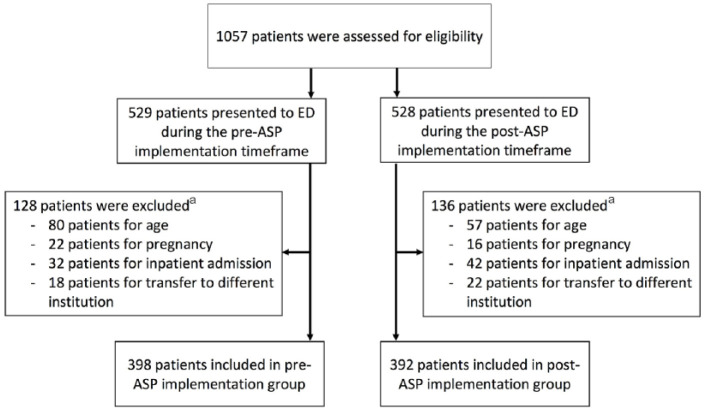
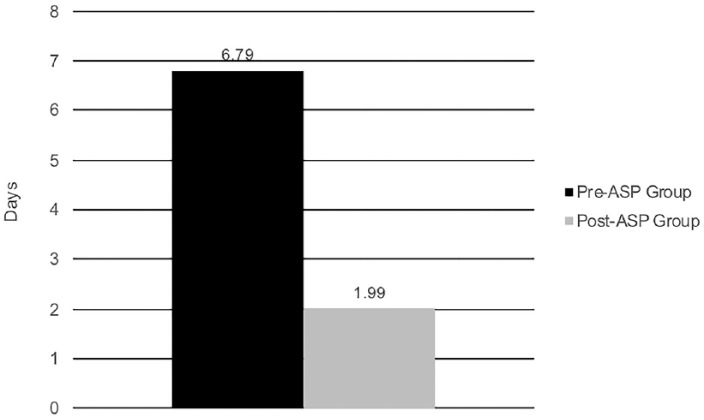
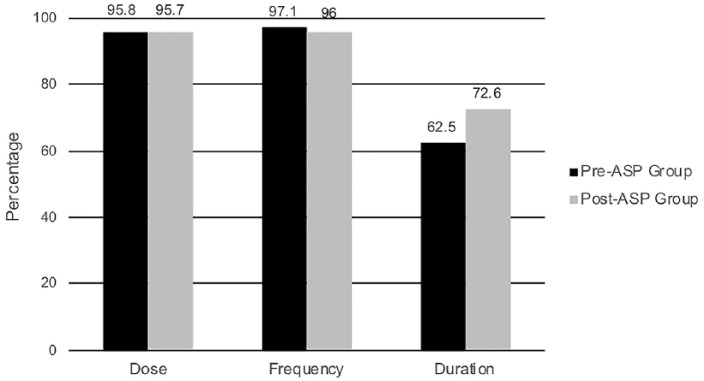
Background: Antimicrobial stewardship programs (ASP) have been widely implemented in hospitals to improve antimicrobial use and prevent resistance. However, the role of ASP in the emergency department (ED) setting is not well defined. Objective: The objective of this study is to evaluate the impact of an ASP pharmacist culture review service in an ED. Methods: This was a retrospective, quasi-experimental study of all patients discharged from the ED with a positive culture. Patients discharged from the ED from February 1, 2015 to October 31, 2015 were managed by ED providers (pre-ASP), and those discharged from February 1, 2016 to October 31, 2016 were managed by a pharmacist-driven ASP (post-ASP implementation). The primary outcome was median time to change of antibiotic(s) in patients with inadequate antimicrobial therapy based on culture results. Secondary outcomes included time to culture evaluation, appropriateness of antimicrobials, and 30-day readmissions. Results: A total of 790 patients were included in the analysis (398 in pre-ASP group vs 392 in post-ASP implementation group). Median time to modification of inadequate antibiotic therapy decreased from 6.79 days in the pre-ASP group to 1.99 days in the post-ASP implementation group (P < .0001). Median time to culture review decreased in the post-ASP implementation group from 9.83 to 0.32 days (P < .0001). Appropriateness of culture-guided therapy increased in the post-ASP implementation group from 85.7 to 91.8% (P = .047). The rate of combined ED revisits and hospital readmissions was similar between groups (P = .367). Conclusion: ASP pharmacist evaluation of positive cultures in the ED was associated with a significant decrease in the time to appropriate therapy in patients discharged with inadequate therapy and higher rates of appropriate antimicrobial therapy.
Keywords: anti-infectives; clinical services; infectious diseases; physician prescribing.
© The Author(s) 2019.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Joint Commission on Hospital Accreditation. Joint Commission joins White House effort to reduce antibiotic overuse. Jt Comm Perspect. 2015;35:4, 11. - PubMed
-
- Department of Health and Human Services. Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities. 42 CFR §483.80. https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare.... Updated October 24, 2016. Accessed January 24 2017.
-
- Joint Commission on Hospital Accreditation. Official publication of Joint Commission requirements: new antimicrobial stewardship standard. Jt Comm Perspect. 2016;36:1-4. - PubMed
-
- Shlaes DM, Gerding DN, John JF, Jr, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the prevention of antimicrobial resistance in hospitals: guidelines for the prevention of antimicrobial resistance in hospitals. Clin Infect Dis. 1997;25:584-599. - PubMed
LinkOut - more resources
Full Text Sources
