

Adjusting iron and vitamin A status in settings of inflammation: a sensitivity analysis of the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) approach
- PMID: 32743650
- PMCID: PMC7396268
- DOI: 10.1093/ajcn/nqaa141
Adjusting iron and vitamin A status in settings of inflammation: a sensitivity analysis of the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) approach
Abstract
Background: Accurate assessment of iron and vitamin A status is needed to inform public health decisions, but most population-level iron and vitamin A biomarkers are independently influenced by inflammation.
Objectives: We aimed to assess the reproducibility of the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) regression approach to adjust iron [ferritin, soluble transferrin receptor (sTfR)] and vitamin A [retinol-binding protein (RBP), retinol] biomarkers for inflammation (α-1-acid glycoprotein and C-reactive protein).
Methods: We conducted a sensitivity analysis comparing unadjusted and adjusted estimates of iron and vitamin A deficiency using the internal-survey regression approach from BRINDA phase 1 (16 surveys in children, 10 surveys in women) and 13 additional surveys for children and women (BRINDA phase 2).
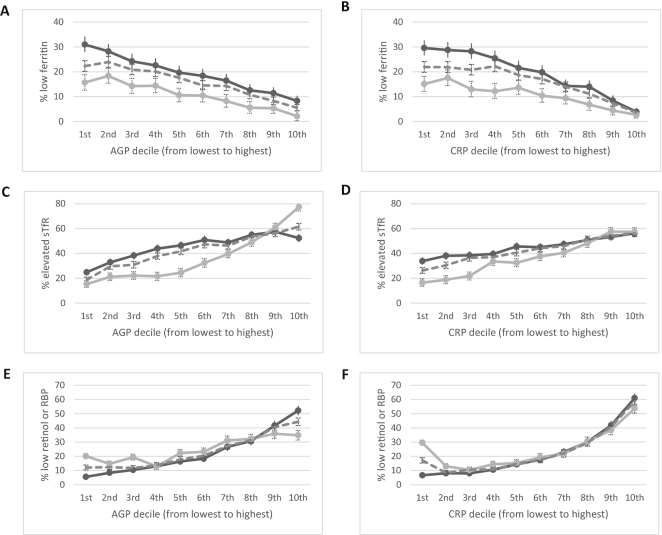
Results: The relations between inflammation and iron or vitamin A biomarkers were statistically significant except for vitamin A biomarkers in women. Heterogeneity of the regression coefficients across surveys was high. Among children, internal-survey adjustments increased the estimated prevalence of depleted iron stores (ferritin <12 µg/L) by a median of 11 percentage points (pp) (24 pp and 9 pp in BRINDA phase 1 and phase 2, respectively), whereas estimates of iron-deficient erythropoiesis (sTfR >8.3 mg/L) decreased by a median of 15 pp (15 pp and 20 pp in BRINDA phase 1 and phase 2, respectively). Vitamin A deficiency (RBP <0.7 µmol/L or retinol <0.7 µmol/L) decreased by a median of 14 pp (18 pp and 8 pp in BRINDA phase 1 and phase 2, respectively) in children. Adjustment for inflammation in women resulted in smaller differences in estimated iron deficiency than in children.
Conclusions: Our findings are consistent with previous BRINDA conclusions that not accounting for inflammation may result in an underestimation of iron deficiency and overestimation of vitamin A deficiency. Research is needed to understand the etiology of the heterogeneity in the regression coefficients before a meta-analyzed regression correction can be considered.
Keywords: biomarkers; inflammation; iron; meta-analysis; micronutrient; nutritional assessment; vitamin A.
Copyright © The Author(s) on behalf of the American Society for Nutrition 2020.
Figures



References
-
- West KP., Jr Vitamin A deficiency disorders in children and women. Food Nutr Bull. 2003;24(4 Suppl):S78–90. - PubMed
-
- Moy RJ. Prevalence, consequences and prevention of childhood nutritional iron deficiency: a child public health perspective. Clin Lab Haematol. 2006;28(5):291–8. - PubMed
-
- Coad J, Conlon C. Iron deficiency in women: assessment, causes and consequences. Curr Opin Clin Nutr Metab Care. 2011;14(6):625–34. - PubMed
-
- Thurnham DI, Northrop-Clewes CA. Inflammation and biomarkers of micronutrient status. Curr Opin Clin Nutr Metab Care. 2016;19(6):458–63. - PubMed
-
- Tomkins A. Assessing micronutrient status in the presence of inflammation. J Nutr. 2003;133(5):1649S–55S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
