

Real-Time Digital Contact Tracing: Development of a System to Control COVID-19 Outbreaks in Nursing Homes and Long-Term Care Facilities
- PMID: 32745013
- PMCID: PMC7451111
- DOI: 10.2196/20828
Real-Time Digital Contact Tracing: Development of a System to Control COVID-19 Outbreaks in Nursing Homes and Long-Term Care Facilities
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can spread rapidly in nursing homes and long-term care (LTC) facilities. Symptoms-based screening and manual contact tracing have limitations that render them ineffective for containing the viral spread in LTC facilities. Symptoms-based screening alone cannot identify asymptomatic people who are infected, and the viral spread is too fast in confined living quarters to be contained by slow manual contact tracing processes.
Objective: We describe the development of a digital contact tracing system that LTC facilities can use to rapidly identify and contain asymptomatic and symptomatic SARS-CoV-2 infected contacts. A compartmental model was also developed to simulate disease transmission dynamics and to assess system performance versus conventional methods.
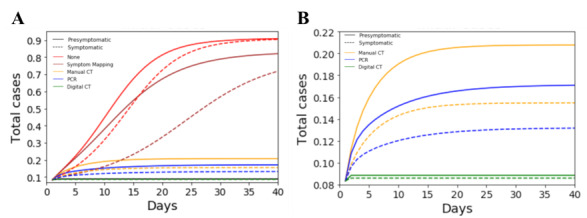
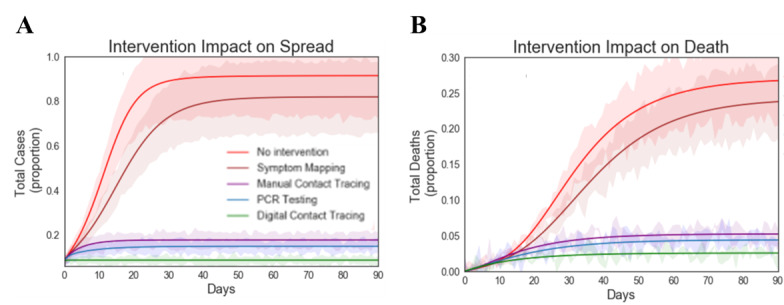
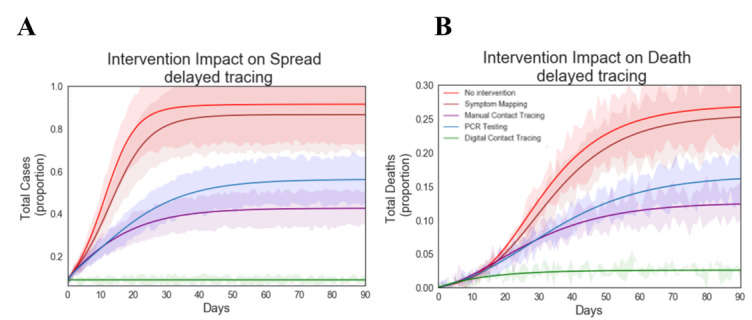
Methods: We developed a compartmental model parameterized specifically to assess the coronavirus disease (COVID-19) transmission in LTC facilities. The model was used to quantify the impact of asymptomatic transmission and to assess the performance of several intervention groups to control outbreaks: no intervention, symptom mapping, polymerase chain reaction testing, and manual and digital contact tracing.
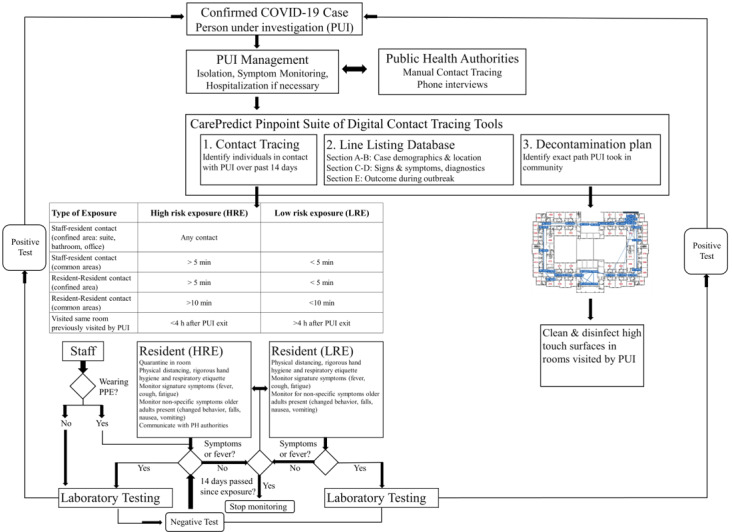
Results: Our digital contact tracing system allows users to rapidly identify and then isolate close contacts, store and track infection data in a respiratory line listing tool, and identify contaminated rooms. Our simulation results indicate that the speed and efficiency of digital contact tracing contributed to superior control performance, yielding up to 52% fewer cases than conventional methods.
Conclusions: Digital contact tracing systems show promise as an effective tool to control COVID-19 outbreaks in LTC facilities. As facilities prepare to relax restrictions and reopen to outside visitors, such tools will allow them to do so in a surgical, cost-effective manner that controls outbreaks while safely giving residents back the life they once had before this pandemic hit.
Keywords: COVID-19; SARS-CoV-2; care homes; contact tracing; digital contact tracing; long term care; nursing homes.
©Gerald Wilmink, Ilyssa Summer, David Marsyla, Subhashree Sukhu, Jeffrey Grote, Gregory Zobel, Howard Fillit, Satish Movva. Originally published in JMIR Public Health and Surveillance (http://publichealth.jmir.org), 25.08.2020.
Conflict of interest statement
Conflicts of Interest: GW, IS, DM, JG, GZ, SS, and SM are employees of CarePredict. HF serves as an advisor to CarePredict corporation.
Figures


References
-
- Provisional Death Counts for Coronavirus Disease 2019 (COVID-19) Centers for Disease Control and Prevention. 2020. https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm.
-
- KFF. https://www.kff.org/
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
