

Role of computed tomography in predicting critical disease in patients with covid-19 pneumonia: A retrospective study using a semiautomatic quantitative method
- PMID: 32745895
- PMCID: PMC7388797
- DOI: 10.1016/j.ejrad.2020.109202
Role of computed tomography in predicting critical disease in patients with covid-19 pneumonia: A retrospective study using a semiautomatic quantitative method
Abstract
Background: So far, only a few studies evaluated the correlation between CT features and clinical outcome in patients with COVID-19 pneumonia.
Purpose: To evaluate CT ability in differentiating critically ill patients requiring invasive ventilation from patients with less severe disease.
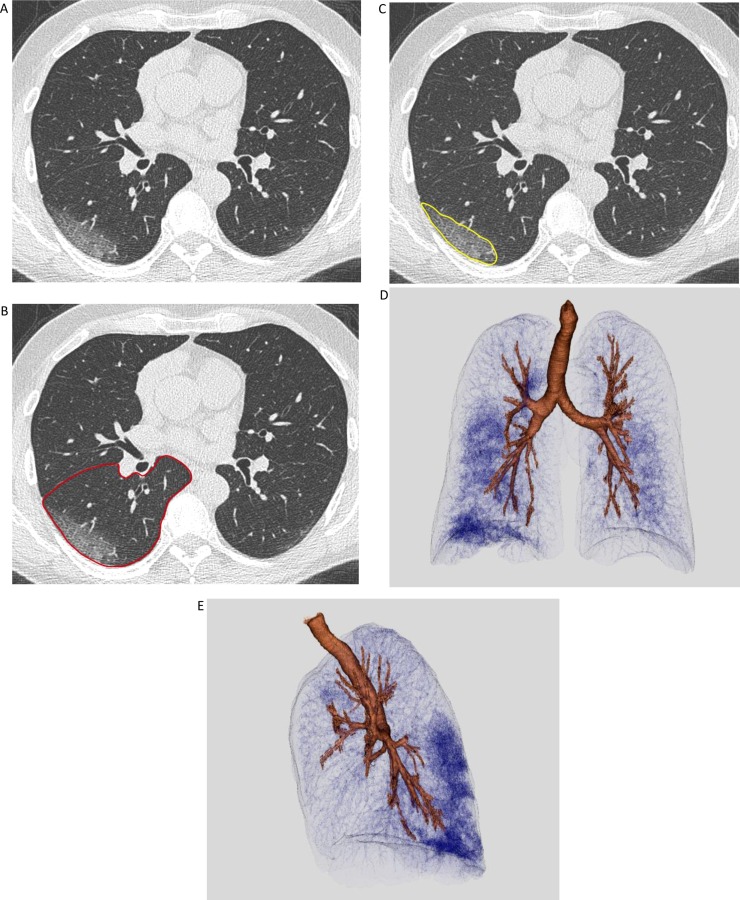
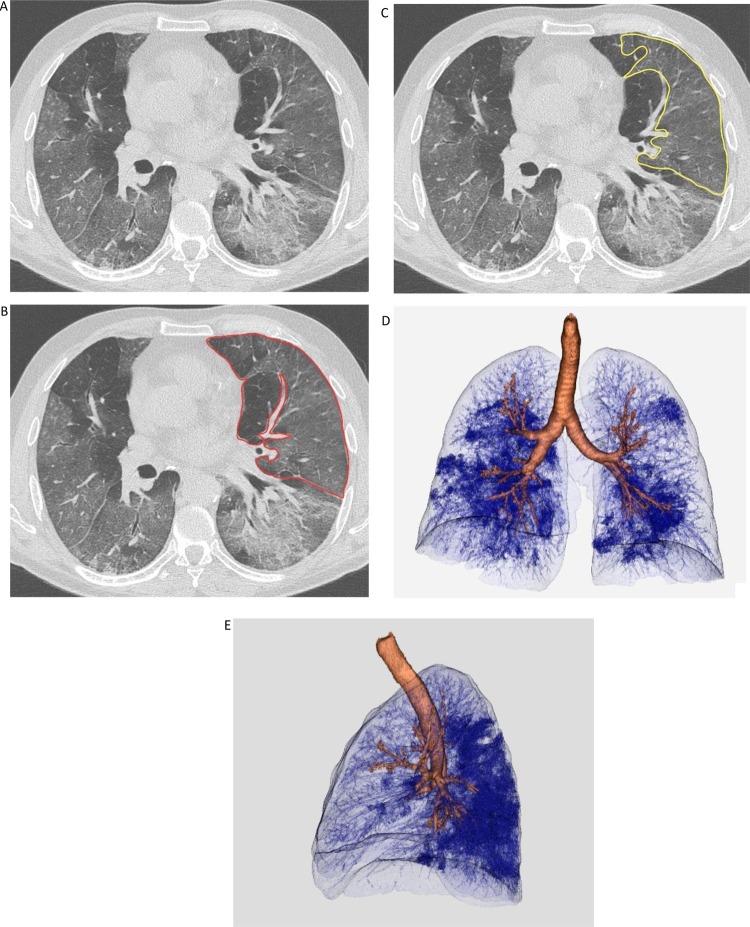
Methods: We retrospectively collected data from patients admitted to our institution for COVID-19 pneumonia between March 5th-24th. Patients were considered critically ill or non-critically ill, depending on the need for mechanical ventilation. CT images from both groups were analyzed for the assessment of qualitative features and disease extension, using a quantitative semiautomatic method. We evaluated the differences between the two groups for clinical, laboratory and CT data. Analyses were conducted on a per-protocol basis.
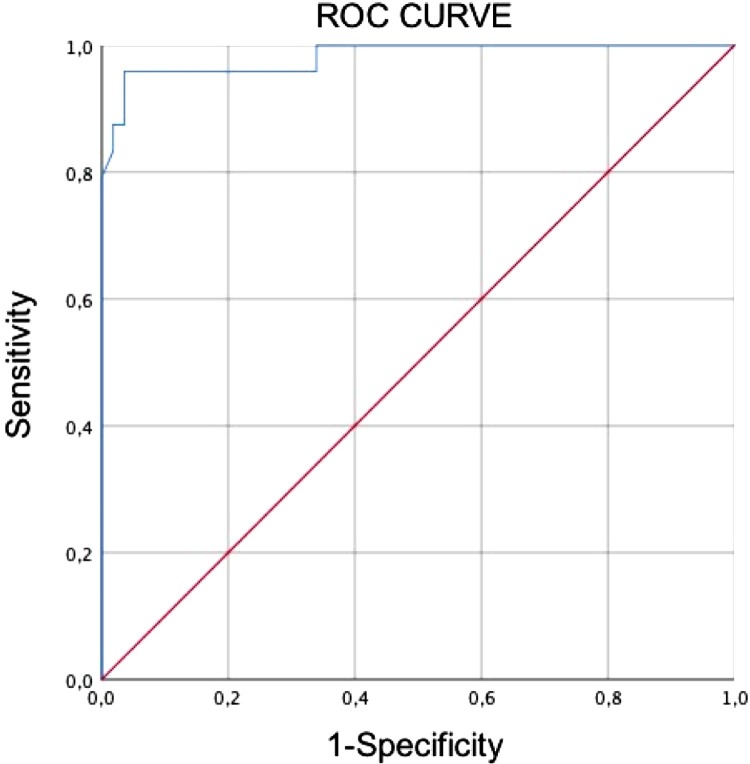
Results: 189 patients were analyzed. PaO2/FIO2 ratio and oxygen saturation (SaO2) were decreased in critically ill patients. At CT, mixed pattern (ground glass opacities (GGO) and consolidation) and GGO alone were more frequent respectively in critically ill and in non-critically ill patients (p < 0.05). Lung volume involvement was significantly higher in critically ill patients (38.5 % vs. 5.8 %, p < 0.05). A cut-off of 23.0 % of lung involvement showed 96 % sensitivity and 96 % specificity in distinguishing critically ill patients from patients with less severe disease. The fraction of involved lung was related to lactate dehydrogenase (LDH) levels, PaO2/FIO2 ratio and SaO2 (p < 0.05).
Conclusion: Lung disease extension, assessed using quantitative CT, has a significant relationship with clinical severity and may predict the need for invasive ventilation in patients with COVID-19.
Keywords: COVID-19; Invasive mechanical ventilation; Lung volume; Pneumonia; Quantitative CT; SARS- CoV-2.
Copyright © 2020 Elsevier B.V. All rights reserved.
Figures
References
-
- 2020. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19 -. 11 March 2020.https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re... (accessed 5 April 2020)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
