

Prevention and Management of Delirium in the Intensive Care Unit
- PMID: 32746469
- PMCID: PMC7855536
- DOI: 10.1055/s-0040-1710572
Prevention and Management of Delirium in the Intensive Care Unit
Abstract
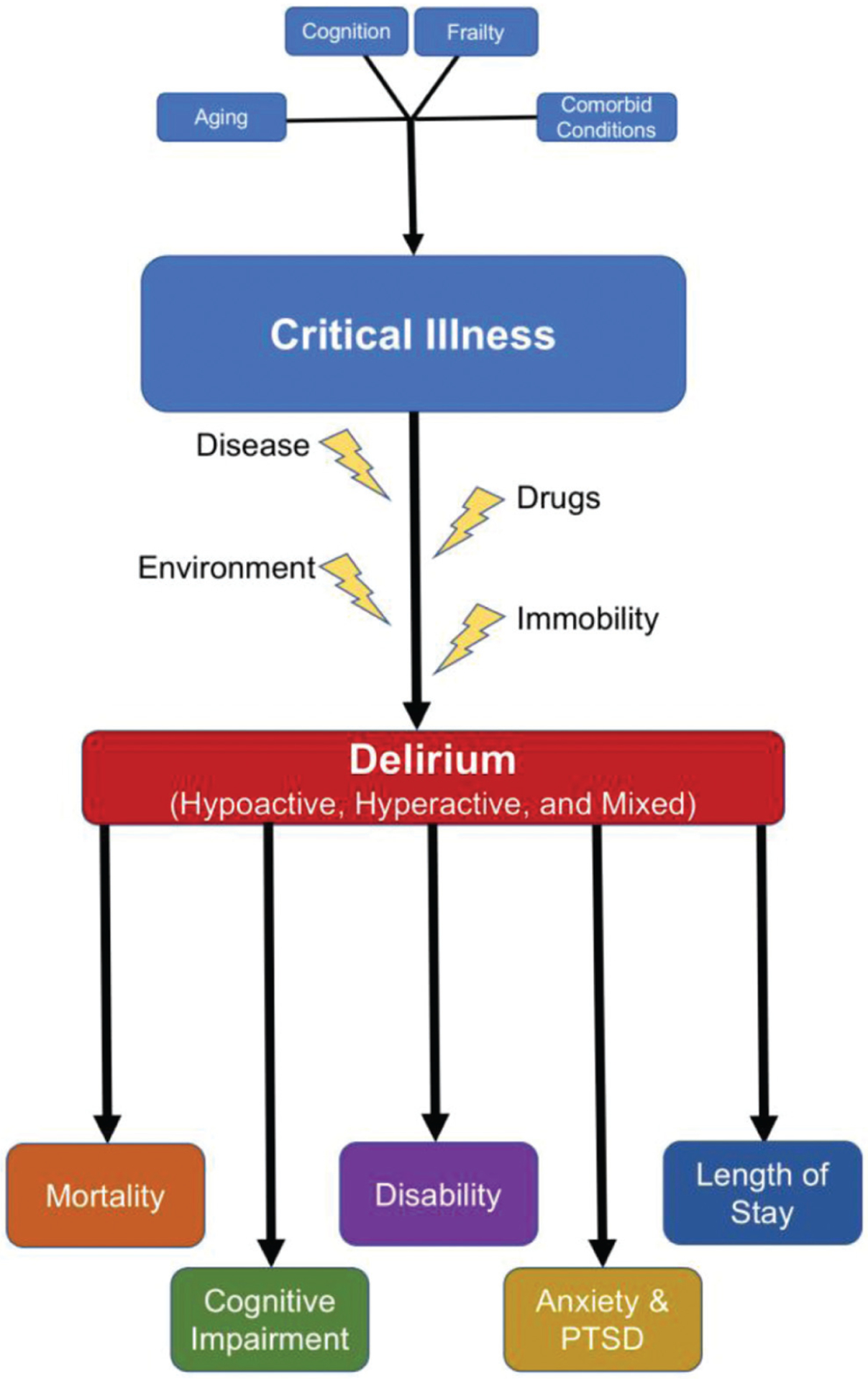
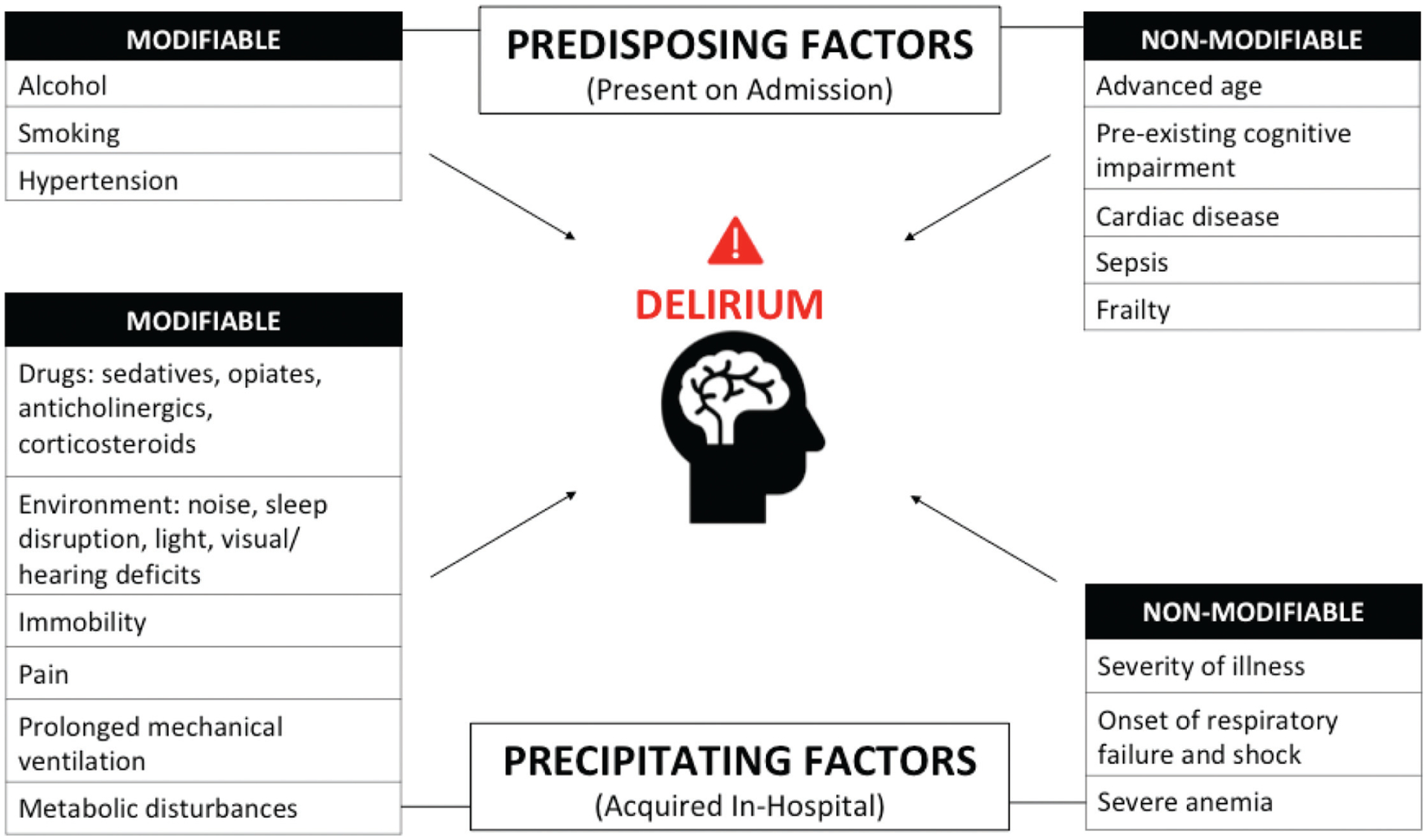
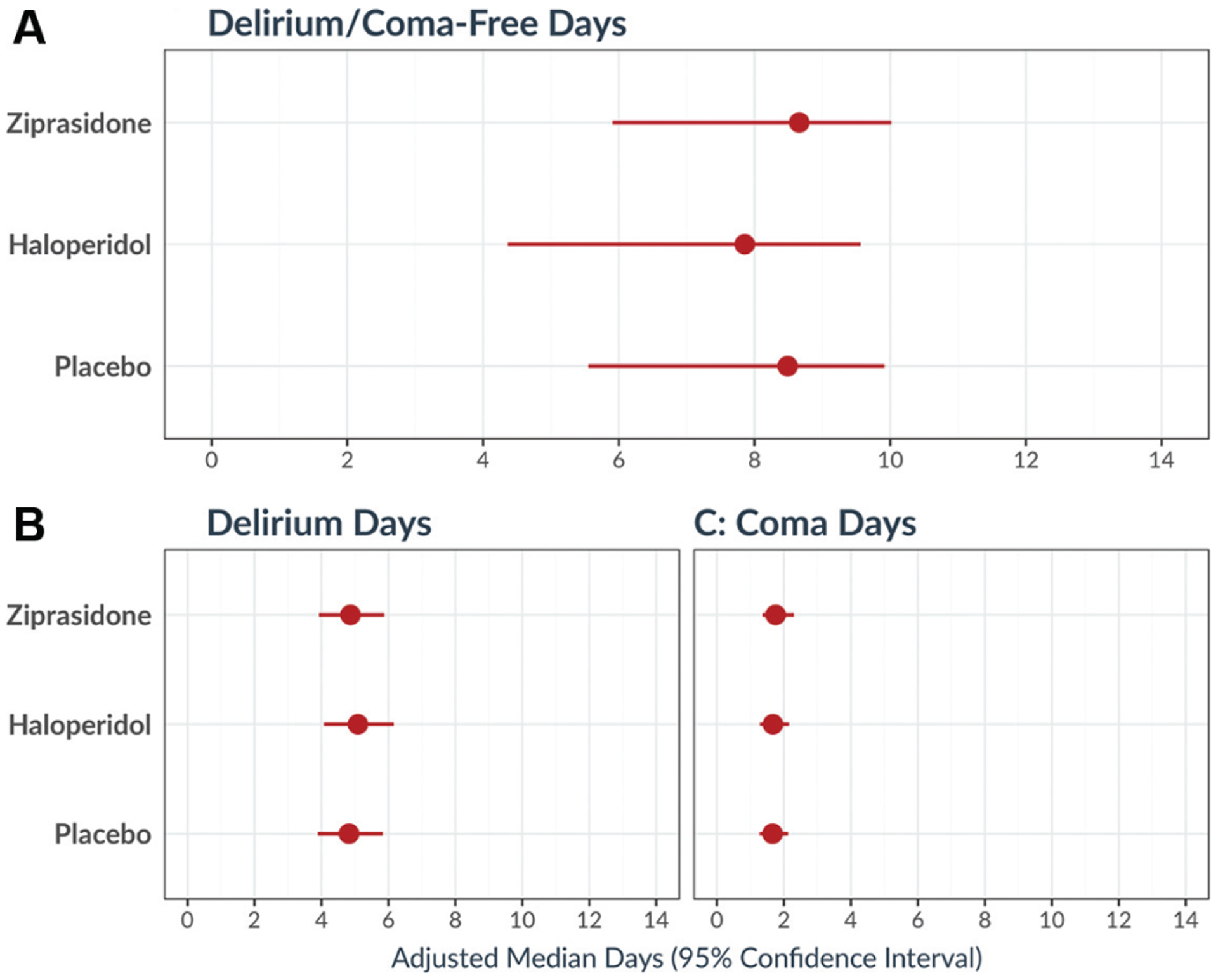
Delirium is a debilitating form of brain dysfunction frequently encountered in the intensive care unit (ICU). It is associated with increased morbidity and mortality, longer lengths of stay, higher hospital costs, and cognitive impairment that persists long after hospital discharge. Predisposing factors include smoking, hypertension, cardiac disease, sepsis, and premorbid dementia. Precipitating factors include respiratory failure and shock, metabolic disturbances, prolonged mechanical ventilation, pain, immobility, and sedatives and adverse environmental conditions impairing vision, hearing, and sleep. Historically, antipsychotic medications were the mainstay of delirium treatment in the critically ill. Based on more recent literature, the current Society of Critical Care Medicine (SCCM) guidelines suggest against routine use of antipsychotics for delirium in critically ill adults. Other pharmacologic interventions (e.g., dexmedetomidine) are under investigation and their impact is not yet clear. Nonpharmacologic interventions thus remain the cornerstone of delirium management. This approach is summarized in the ABCDEF bundle (Assess, prevent, and manage pain; Both SAT and SBT; Choice of analgesia and sedation; Delirium: assess, prevent, and manage; Early mobility and exercise; Family engagement and empowerment). The implementation of this bundle reduces the odds of developing delirium and the chances of needing mechanical ventilation, yet there are challenges to its implementation. There is an urgent need for ongoing studies to more effectively mitigate risk factors and to better understand the pathobiology underlying ICU delirium so as to identify additional potential treatments. Further refinements of therapeutic options, from drugs to rehabilitation, are current areas ripe for study to improve the short- and long-term outcomes of critically ill patients with delirium.
Thieme. All rights reserved.
Conflict of interest statement
None declared.
Figures

References
-
- Celsus AC, Spencer WG. On Medicine [electronic resource]/with an English Translation by Spencer WG. Cambridge, MA: Harvard University Press; 2014
-
- Dubois MJ, Bergeron N, Dumont M, Dial S, Skrobik Y. Delirium in an intensive care unit: a study of risk factors. Intensive Care Med 2001;27(08):1297–1304 - PubMed
-
- Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the Confusion Assessment Method for the intensive care unit (CAM-ICU). JAMA 2001;286(21):2703–2710 - PubMed
-
- Pisani MA, Murphy TE, Van Ness PH, Araujo KL, Inouye SK. Characteristics associated with delirium in older patients in a medical intensive care unit. Arch Intern Med 2007;167(15):1629–1634 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
