

Decreased Incidence of Methicillin-Resistant Staphylococcus aureus Bacteremia in Intensive Care Units: a 10-Year Clinical, Microbiological, and Genotypic Analysis in a Tertiary Hospital
- PMID: 32747360
- PMCID: PMC7508613
- DOI: 10.1128/AAC.01082-20
Decreased Incidence of Methicillin-Resistant Staphylococcus aureus Bacteremia in Intensive Care Units: a 10-Year Clinical, Microbiological, and Genotypic Analysis in a Tertiary Hospital
Abstract
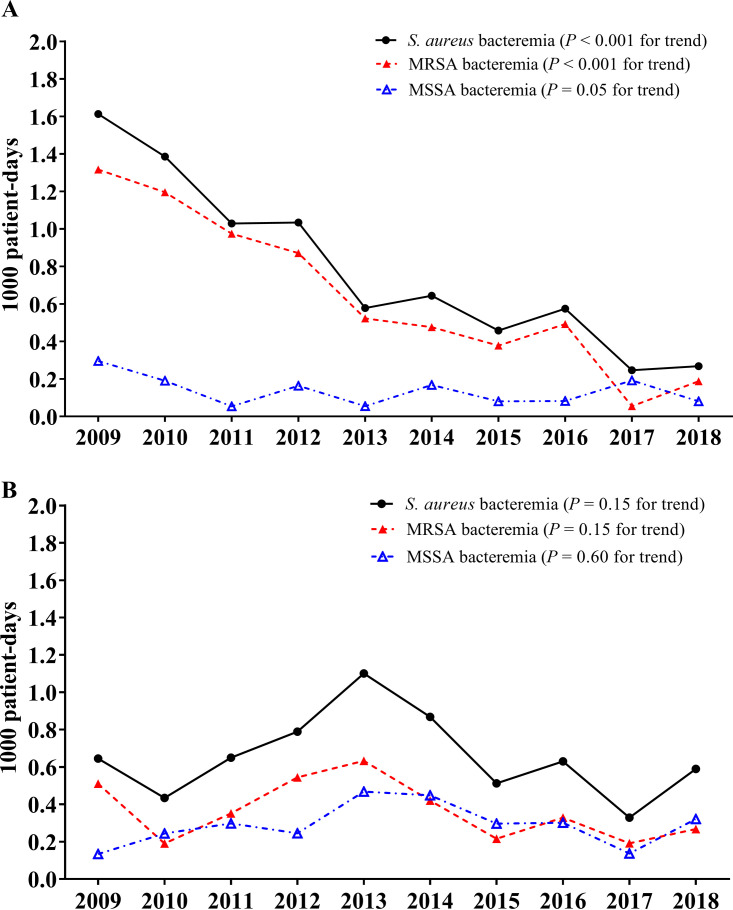
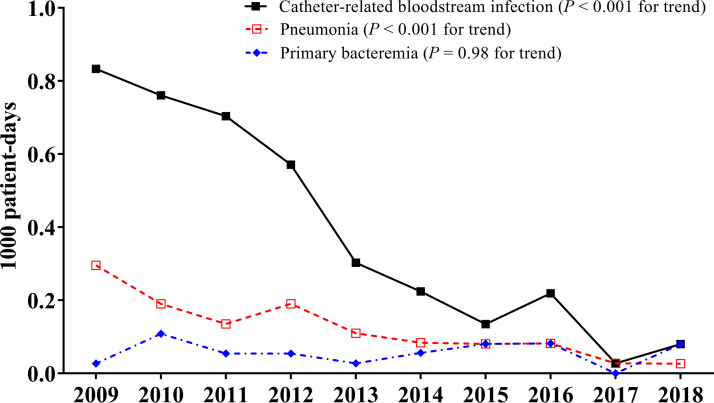
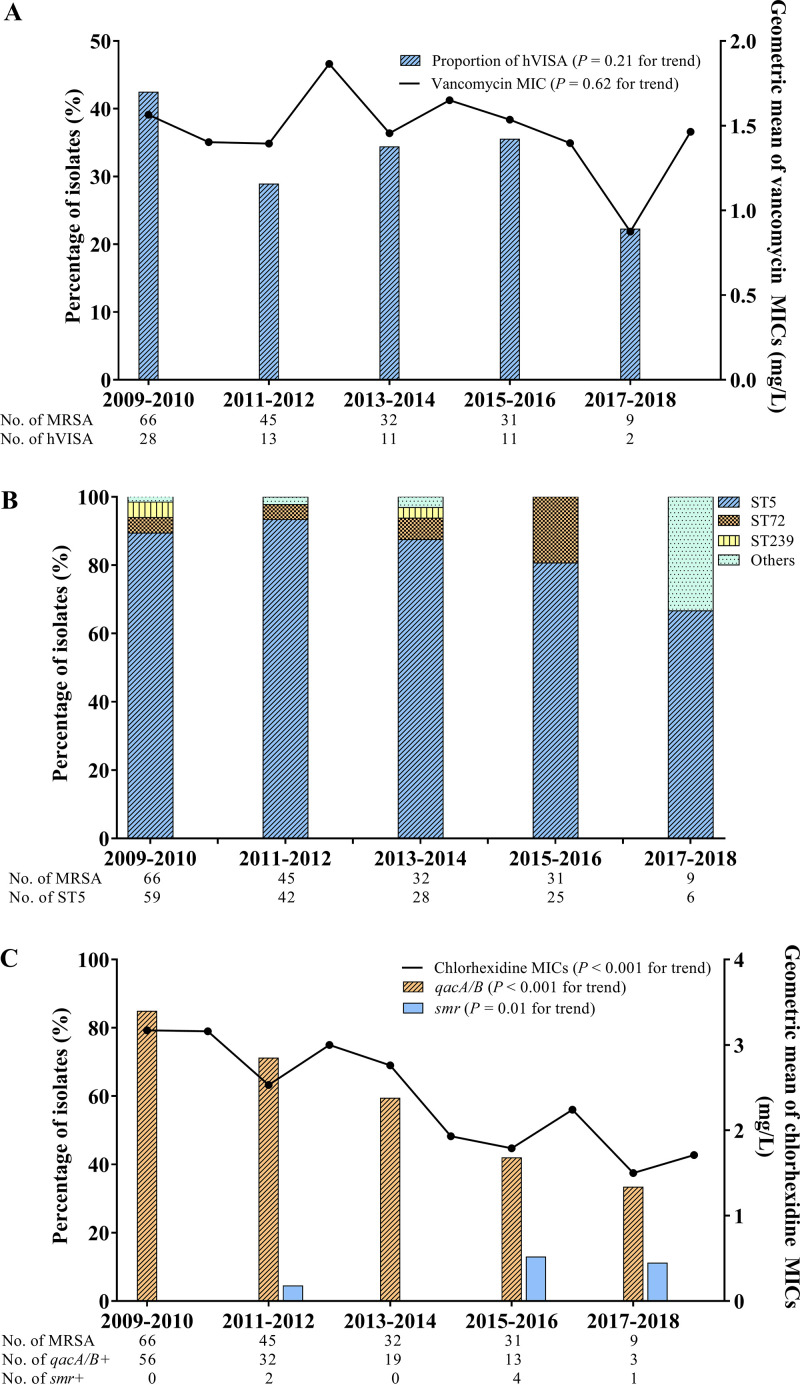
There are limited long-term data on the trends in incidence and characteristics of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia (MRSAB) in intensive care units (ICUs) in which infection control measures have been adopted. We evaluated the trend of incidence and changes in characteristics of MRSA bacteremia in ICUs at a tertiary-care hospital over 10 years using prospective cohort data. ICU-acquired bacteremia was defined as S. aureus bacteremia (SAB) that occurred 48 h or more after ICU admission. MRSA isolates were collected and subjected to microbiological and genotypic analyses. A total of 529 SAB episodes were identified among 367,175 ICU patients. Of these episodes, 288 (54.4%) were ICU acquired, 238 (82.6%) of which were MRSAB. The incidence density of ICU-acquired MRSAB decreased from 1.32 per 1,000 patient-days to 0.19 per 1,000 patient-days (a decrease of 20% annually; P < 0.001 for trend), whereas that of non-ICU-acquired MRSAB fluctuated and did not decrease significantly. The decline in ICU-acquired MRSAB was due to lower catheter-related infection and less pneumonia. Rates of persistent bacteremia and 12-week mortality also fell significantly. A total of 183 isolates were collected from 238 ICU-acquired MRSAB cases. There were no significant changes in the geometric means of vancomycin MICs, vancomycin heteroresistance, or the sequence types of MRSA isolates over time. Chlorhexidine MICs decreased (P < 0.001 for trend) in association with a decline in frequency of the qacA or qacB gene that was related to reductions in specific spa types. The incidence of MRSAB in ICUs has decreased dramatically over time, but most of the microbiological and genotypic characteristics of MRSA isolates have not changed.
Keywords: bacteremia; genotype; incidence; intensive care unit; methicillin-resistant Staphylococcus aureus; vancomycin MIC.
Copyright © 2020 American Society for Microbiology.
Figures
Similar articles
-
Clinical impact of and microbiological risk factors for qacA/B positivity in ICU-acquired ST5-methicillin-resistant SCCmec type II Staphylococcus aureus bacteremia.Sci Rep. 2022 Jul 6;12(1):11413. doi: 10.1038/s41598-022-15546-3. Sci Rep. 2022. PMID: 35794229 Free PMC article.
-
Clinical and Molecular Characteristics of qacA- and qacB-Positive Methicillin-Resistant Staphylococcus aureus Causing Bloodstream Infections.Antimicrob Agents Chemother. 2019 Mar 27;63(4):e02157-18. doi: 10.1128/AAC.02157-18. Print 2019 Apr. Antimicrob Agents Chemother. 2019. PMID: 30718251 Free PMC article.
-
Methicillin-resistant Staphylococcus aureus central line-associated bloodstream infections in US intensive care units, 1997-2007.JAMA. 2009 Feb 18;301(7):727-36. doi: 10.1001/jama.2009.153. JAMA. 2009. PMID: 19224749
-
Ceftaroline for the treatment of methicillin-resistant Staphylococcus aureus bacteremia.Am J Health Syst Pharm. 2017 Feb 15;74(4):201-208. doi: 10.2146/ajhp160006. Am J Health Syst Pharm. 2017. PMID: 28179245 Review.
-
Association between high vancomycin minimum inhibitory concentration and clinical outcomes in patients with methicillin-resistant Staphylococcus aureus bacteremia: a meta-analysis.Infection. 2021 Oct;49(5):803-811. doi: 10.1007/s15010-020-01568-4. Epub 2021 Jan 4. Infection. 2021. PMID: 33394368 Review.
Cited by
-
Changing Epidemiology of Pathogenic Bacteria Over the Past 20 Years in Korea.J Korean Med Sci. 2023 Mar 13;38(10):e73. doi: 10.3346/jkms.2023.38.e73. J Korean Med Sci. 2023. PMID: 36918027 Free PMC article.
-
Emergence of eravacycline heteroresistance in carbapenem-resistant Acinetobacter baumannii isolates in China.Front Cell Infect Microbiol. 2024 Mar 27;14:1356353. doi: 10.3389/fcimb.2024.1356353. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38601741 Free PMC article.
-
Exploiting the Zebrafish Model for Sepsis Research: Insights into Pathophysiology and Therapeutic Potentials.Drug Des Devel Ther. 2024 Nov 22;18:5333-5349. doi: 10.2147/DDDT.S500276. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 39600867 Free PMC article. Review.
-
Clinical impact of and microbiological risk factors for qacA/B positivity in ICU-acquired ST5-methicillin-resistant SCCmec type II Staphylococcus aureus bacteremia.Sci Rep. 2022 Jul 6;12(1):11413. doi: 10.1038/s41598-022-15546-3. Sci Rep. 2022. PMID: 35794229 Free PMC article.
-
Overexpression of KPC contributes to ceftazidime-avibactam heteroresistance in clinical isolates of carbapenem-resistant Klebsiella pneumoniae.Front Cell Infect Microbiol. 2024 Dec 6;14:1450530. doi: 10.3389/fcimb.2024.1450530. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39711783 Free PMC article.
References
-
- Jain R, Kralovic SM, Evans ME, Ambrose M, Simbartl LA, Obrosky DS, Render ML, Freyberg RW, Jernigan JA, Muder RR, Miller LJ, Roselle GA. 2011. Veterans Affairs initiative to prevent methicillin-resistant Staphylococcus aureus infections. N Engl J Med 364:1419–1430. doi:10.1056/NEJMoa1007474. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
