

Meta-analysis of interventions to reduce door to needle times in acute ischaemic stroke patients
- PMID: 32747390
- PMCID: PMC7401993
- DOI: 10.1136/bmjoq-2020-000915
Meta-analysis of interventions to reduce door to needle times in acute ischaemic stroke patients
Abstract
Background: Door-to-needle time (DTN) has an important impact on thrombolysis and reperfusion outcomes in the treatment of acute ischaemic stroke. This systematic review is a critical synthesis of studies evaluating DTN reduction strategies.
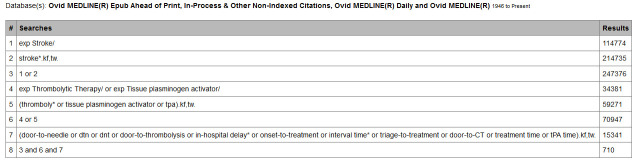
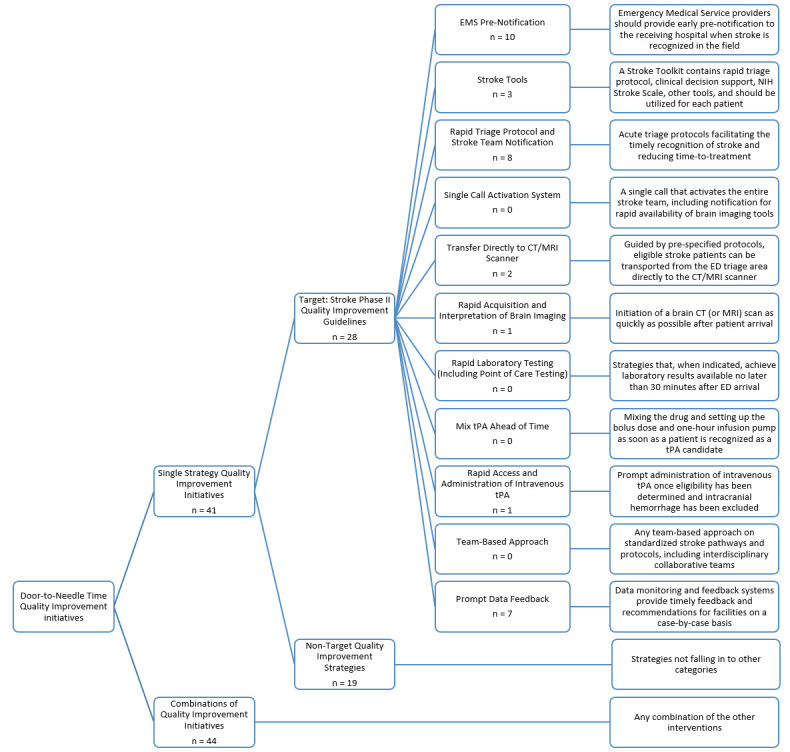
Method: Ovid MEDLINE, PubMed, Cochrane Database of Systematic Reviews, CINAHL, ProQuest dissertations and LILACS were used as bibliographic databases for primary literature. CIHI, Health Quality Council of Alberta, Health Quality Ontario and websites of heart and stroke associations in Canada, USA, UK, Australia and New Zealand were used as sources of grey literature. Searched reports were screened by title and abstract, and full texts were located for review. Articles quality was evaluated using National Institute of Health's Study Quality Assessment tools. Methods for improving DTN were categorised under 13 DTN reduction strategies, primarily adapted from the Target: Stroke Phase II recommendations, and including two additional categories: Strategies not encompassed by any Target: Stroke recommendation, and Combinations of Interventions.
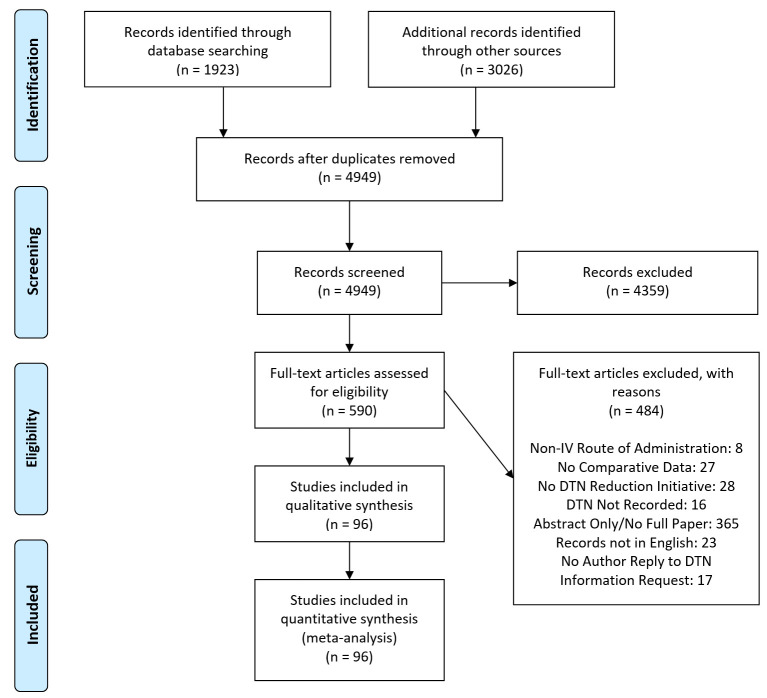
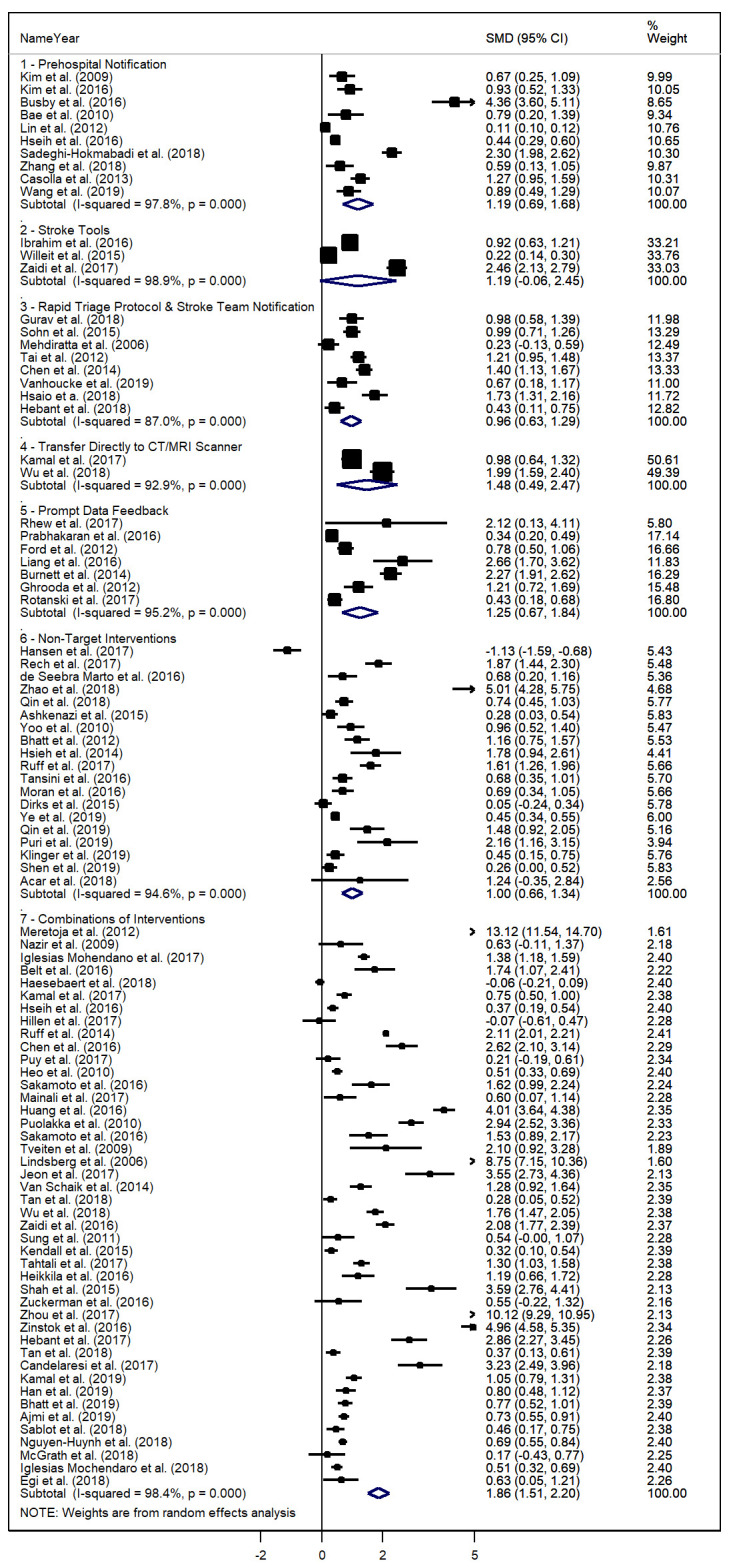
Results: 96 studies (4 randomised control trials, 1 review, 91 observational pre/post studies) were included in the review. All strategies and interventions resulted in a reduction of DTN. Approaches using combinations of interventions were the most effective at reducing DTN (33.77% DTN reduction, standard mean difference=1.857, 95% CI=1.510-2.205), and were more effective than approaches using only a single strategy (p=0.040). DTN reduction was associated with the duration of the DTN reduction programme at each facility (p=0.006).
Interpretation: The greatest reductions in DTN were observed when implementing combinations of DTN reduction strategies, although there was no significant advantage to implementing more than two strategies simultaneously.
Prospero registration number: 42016036215.
Keywords: efficiency; emergency department; organizational; quality improvement.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MS reports grants from Alberta Health Services rewarded for the 2016 Systematic Review Grant Competition, during the conduct of the study. MH reports personal fees from Merck, non-financial support from Hoffmann-La Roche Canada Ltd, grants from Covidien (Medtronic), grants from Boehringer-Ingleheim, grants from Stryker Inc., grants from Medtronic LLC, grants from NoNO Inc., outside the submitted work. In addition, MH has a patent Systems and Methods for Assisting in Decision-Making and Triaging for Acute Stroke Patients issued to US Patent office Number: 62/086,077 and owns stock in Calgary Scientific Incorporated, a company that focuses on medical imaging software, is a director of the Canadian Federation of Neurological Sciences, a not-for-profit group, is a director of Circle NeuroVascular Inc. and has received grant support from Alberta Innovates Health Solutions, CIHR, Heart & Stroke Foundation of Canada, National Institutes of Neurological Disorders and Stroke.
Figures
References
-
- Hacke W, Kaste M, Fieschi C, et al. . Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European cooperative acute stroke study (ECASS). JAMA 1995;274:1017–25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical