

Major GI bleeding in older persons using aspirin: incidence and risk factors in the ASPREE randomised controlled trial
- PMID: 32747412
- PMCID: PMC7957959
- DOI: 10.1136/gutjnl-2020-321585
Major GI bleeding in older persons using aspirin: incidence and risk factors in the ASPREE randomised controlled trial
Abstract
Objective: There is a lack of robust data on significant gastrointestinal bleeding in older people using aspirin. We calculated the incidence, risk factors and absolute risk using data from a large randomised, controlled trial.
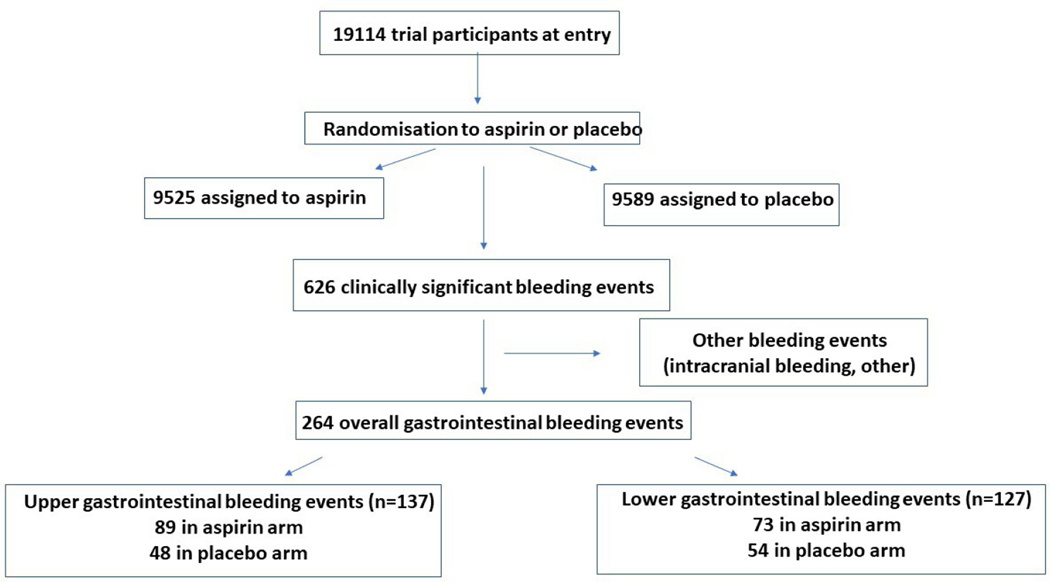
Design: Data were extracted from an aspirin versus placebo primary prevention trial conducted throughout 2010-2017 ('ASPirin in Reducing Events in the Elderly (ASPREE)', n=19 114) in community-dwelling persons aged ≥70 years. Clinical characteristics were collected at baseline and annually. The endpoint was major GI bleeding that resulted in transfusion, hospitalisation, surgery or death, adjudicated independently by two physicians blinded to trial arm.
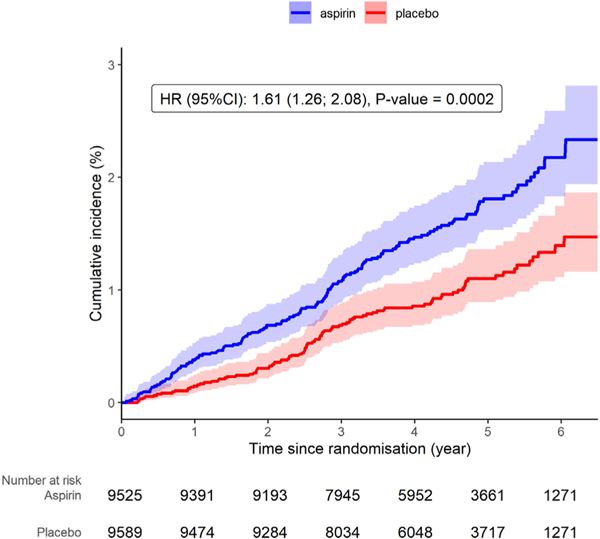
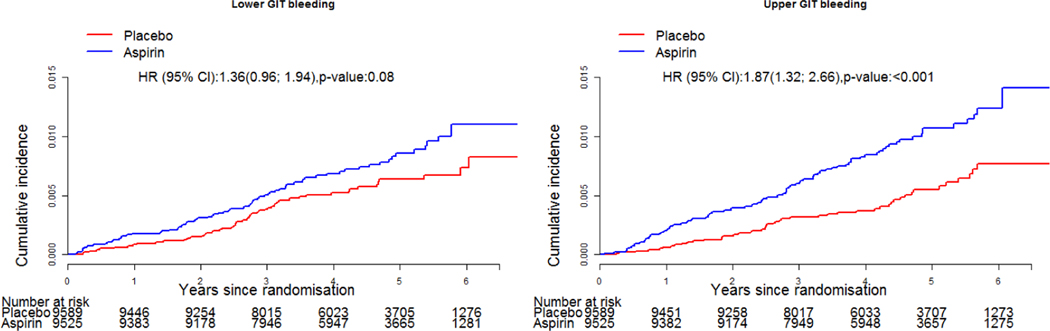
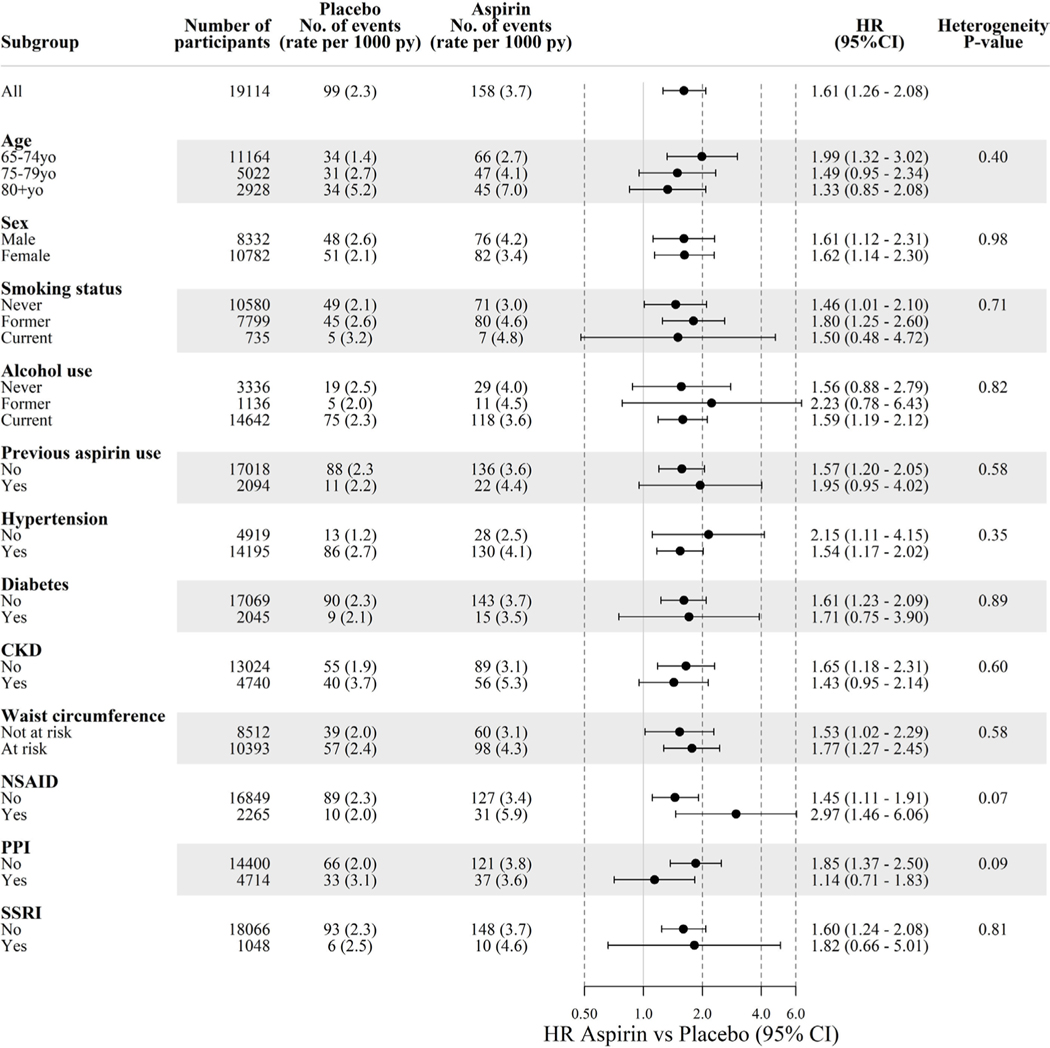
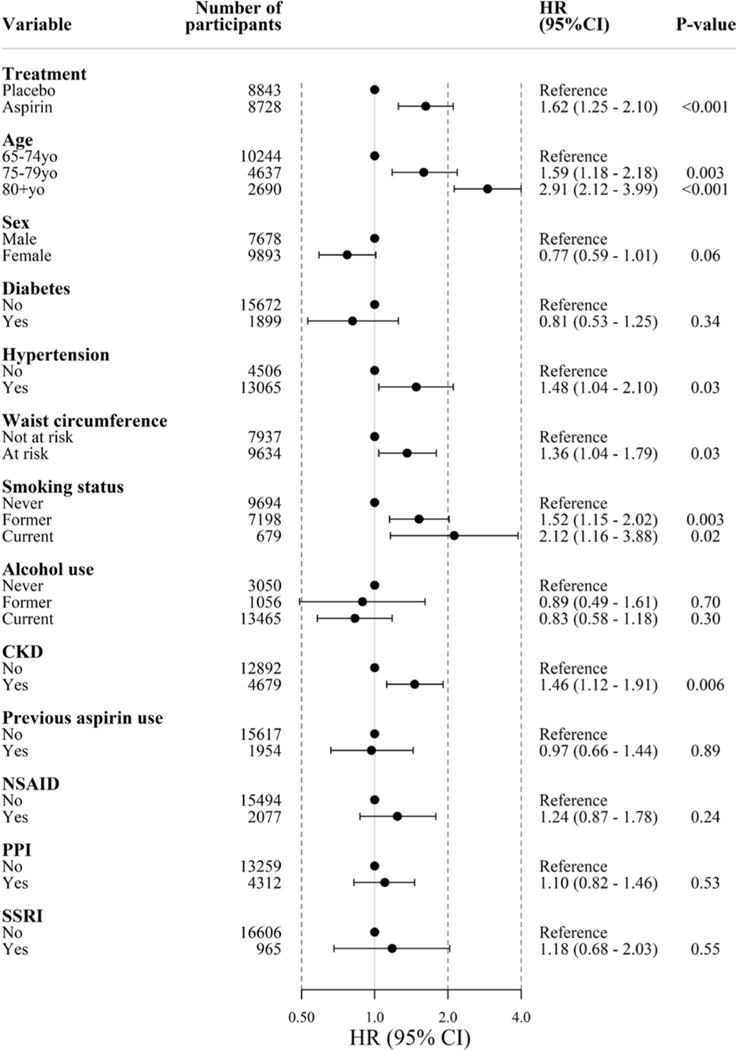
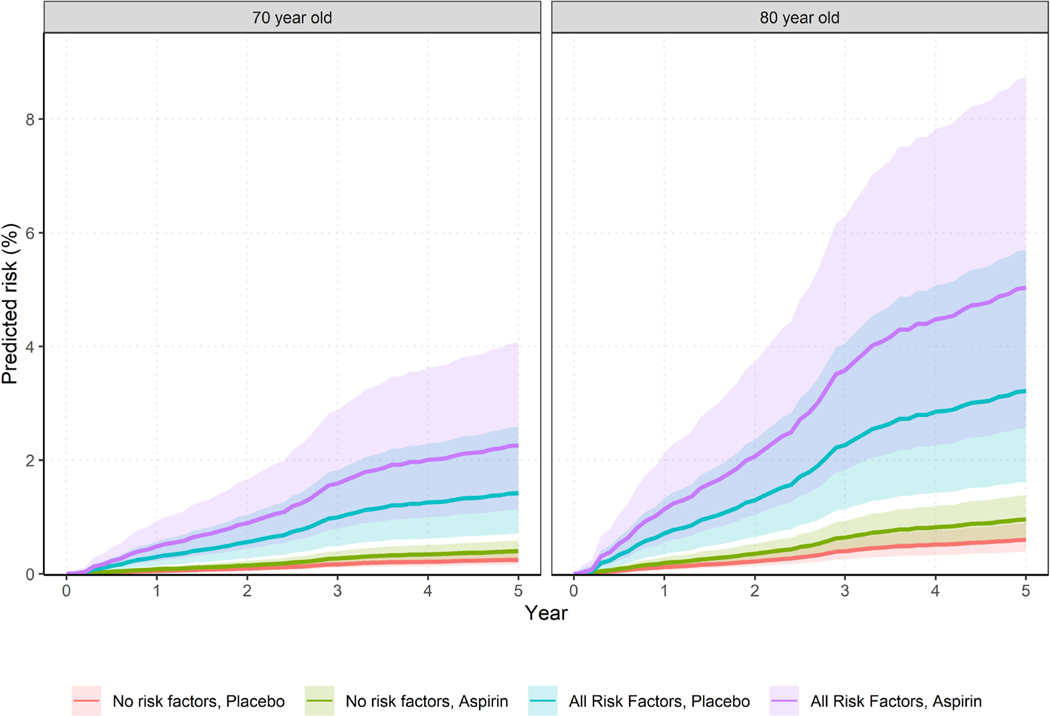
Results: Over a median follow-up of 4.7 years (88 389 person years), there were 137 upper GI bleeds (89 in aspirin arm and 48 in placebo arm, HR 1.87, 95% CI 1.32 to 2.66, p<0.01) and 127 lower GI bleeds (73 in aspirin and 54 in placebo arm, HR 1.36, 95% CI 0.96 to 1.94, p=0.08) reflecting a 60% increase in bleeding overall. There were two fatal bleeds in the placebo arm. Multivariable analyses indicated age, smoking, hypertension, chronic kidney disease and obesity increased bleeding risk. The absolute 5-year risk of bleeding was 0.25% (95% CI 0.16% to 0.37%) for a 70 year old not on aspirin and up to 5.03% (2.56% to 8.73%) for an 80 year old taking aspirin with additional risk factors.
Conclusion: Aspirin increases overall GI bleeding risk by 60%; however, the 5-year absolute risk of serious bleeding is modest in younger, well individuals. These data may assist patients and their clinicians to make informed decisions about prophylactic use of aspirin.
Trial registration number: ASPREE. NCT01038583.
Keywords: aspirin; clinical trials; elderly; epidemiology; gastrointestinal bleeding.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Daily aspirin for primary prevention increased risk for major GI bleeding in healthy older adults.Ann Intern Med. 2021 Jan;174(1):JC4. doi: 10.7326/ACPJ202101190-004. Epub 2021 Jan 5. Ann Intern Med. 2021. PMID: 33395330
References
-
- Whitlock EP, Burda BU, Williams SB, et al. Bleeding risks with aspirin use for primary prevention in adults: a systematic review for the U.S. preventive services Task force. Ann Intern Med 2016;164:826–35. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical