

Reducing Antibiotic Prescribing in Primary Care for Respiratory Illness
- PMID: 32747473
- PMCID: PMC7461202
- DOI: 10.1542/peds.2020-0038
Reducing Antibiotic Prescribing in Primary Care for Respiratory Illness
Abstract
Background: One-third of outpatient antibiotic prescriptions for pediatric acute respiratory tract infections (ARTIs) are inappropriate. We evaluated a distance learning program's effectiveness for reducing outpatient antibiotic prescribing for ARTI visits.
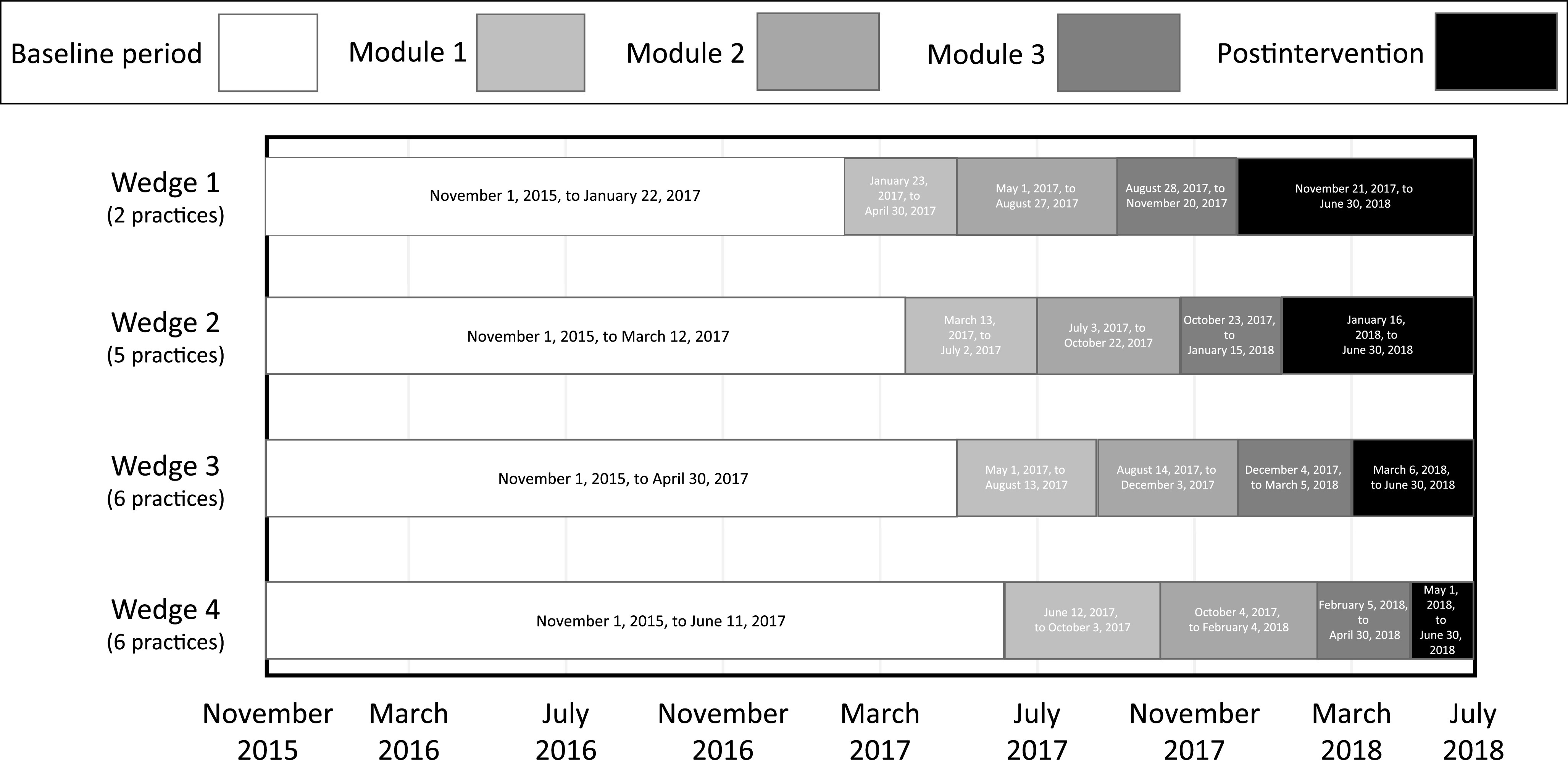
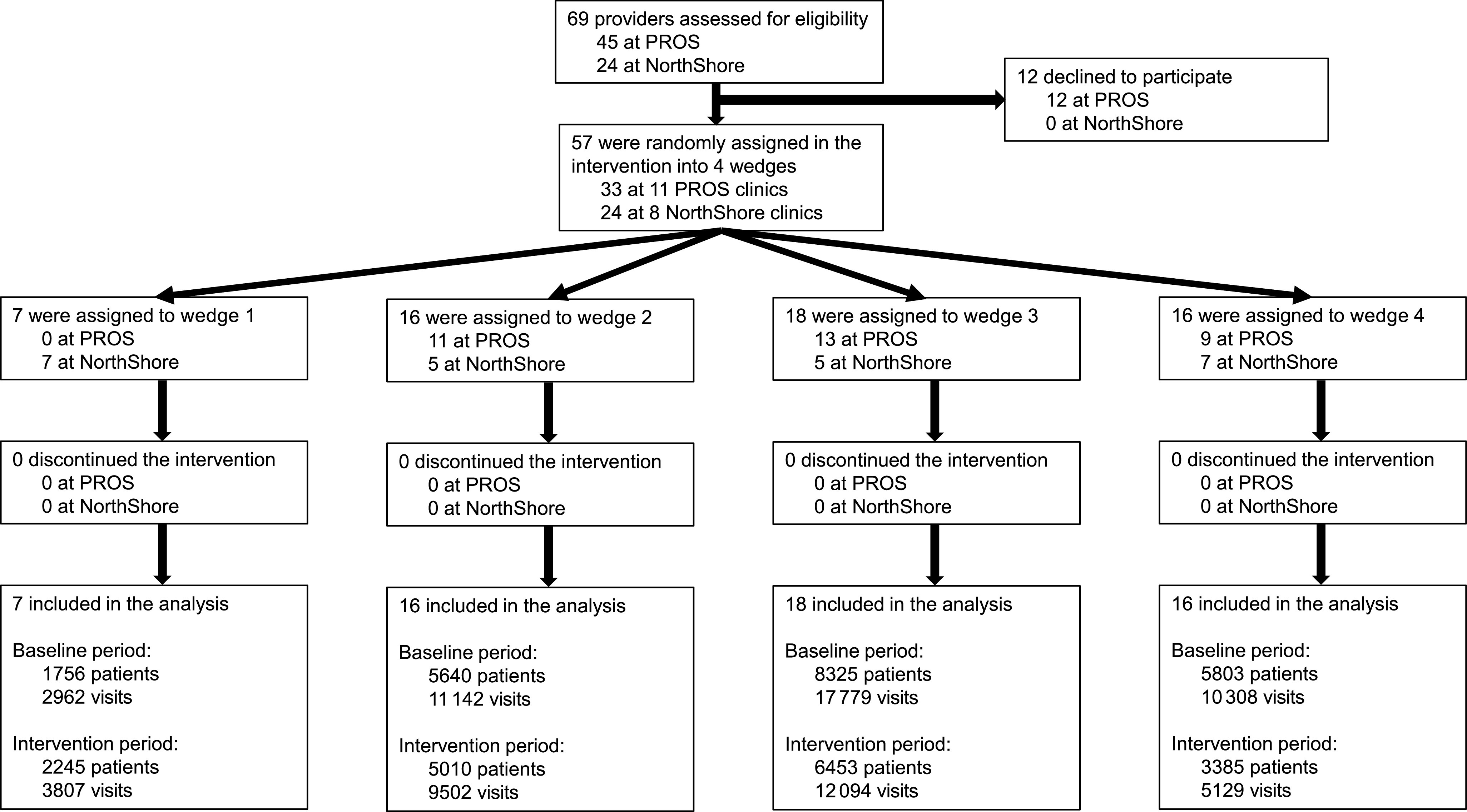
Methods: In this stepped-wedge clinical trial run from November 2015 to June 2018, we randomly assigned 19 pediatric practices belonging to the Pediatric Research in Office Settings Network or the NorthShore University HealthSystem to 4 wedges. Visits for acute otitis media, bronchitis, pharyngitis, sinusitis, and upper respiratory infection for children 6 months to <11 years old without recent antibiotic use were included. Clinicians received the intervention as 3 program modules containing online tutorials and webinars on evidence-based communication strategies and antibioti c prescribing, booster video vignettes, and individualized antibiotic prescribing feedback reports over 11 months. The primary outcome was overall antibiotic prescribing rates for all ARTI visits. Mixed-effects logistic regression compared prescribing rates during each program module and a postintervention period to a baseline control period. Odds ratios were converted to adjusted rate ratios (aRRs) for interpretability.
Results: Among 72 723 ARTI visits by 29 762 patients, intention-to-treat analyses revealed a 7% decrease in the probability of antibiotic prescribing for ARTI overall between the baseline and postintervention periods (aRR 0.93; 95% confidence interval [CI], 0.90-0.96). Second-line antibiotic prescribing decreased for streptococcal pharyngitis (aRR 0.66; 95% CI, 0.50-0.87) and sinusitis (aRR 0.59; 95% CI, 0.44-0.77) but not for acute otitis media (aRR 0.93; 95% CI, 0.83-1.03). Any antibiotic prescribing decreased for viral ARTIs (aRR 0.60; 95% CI, 0.51-0.70).
Conclusions: This program reduced antibiotic prescribing during outpatient ARTI visits; broader dissemination may be beneficial.
Trial registration: ClinicalTrials.gov NCT02943551.
Copyright © 2020 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Comment in
-
The Key to Antibiotic Stewardship Is Combining Interventions.Pediatrics. 2020 Sep;146(3):e2020012922. doi: 10.1542/peds.2020-012922. Epub 2020 Aug 3. Pediatrics. 2020. PMID: 32747474 No abstract available.
References
-
- Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128(6):1053–1061 - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. . Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA. 2016;315(17):1864–1873 - PubMed
-
- Kronman MP, Zhou C, Mangione-Smith R. Bacterial prevalence and antimicrobial prescribing trends for acute respiratory tract infections. Pediatrics. 2014;134(4). Available at: www.pediatrics.org/cgi/content/full/134/4/e956 - PubMed
-
- Centers for Disease Control and Prevention. National action plan for combating antibiotic-resistant bacteria. Available at: https://www.cdc.gov/drugresistance/pdf/national_action_plan_for_combatin.... Accessed March 14, 2019
