

Bariatric surgery reveals a gut-restricted TGR5 agonist with anti-diabetic effects
- PMID: 32747812
- PMCID: PMC7891870
- DOI: 10.1038/s41589-020-0604-z
Bariatric surgery reveals a gut-restricted TGR5 agonist with anti-diabetic effects
Abstract
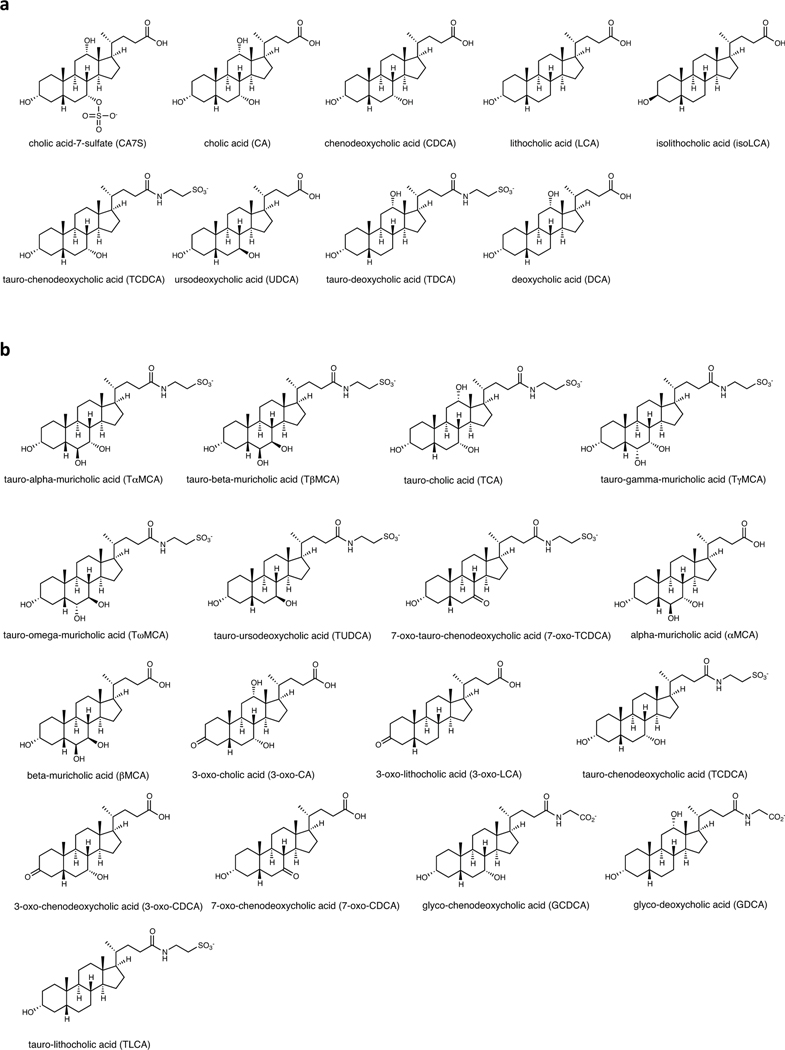
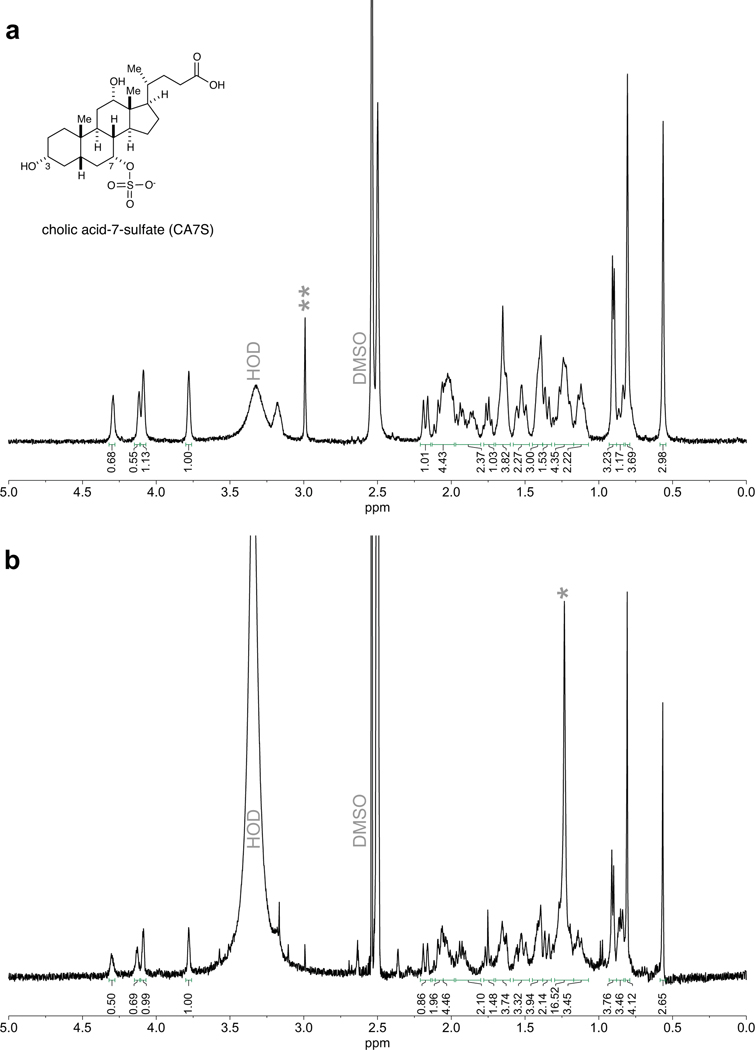
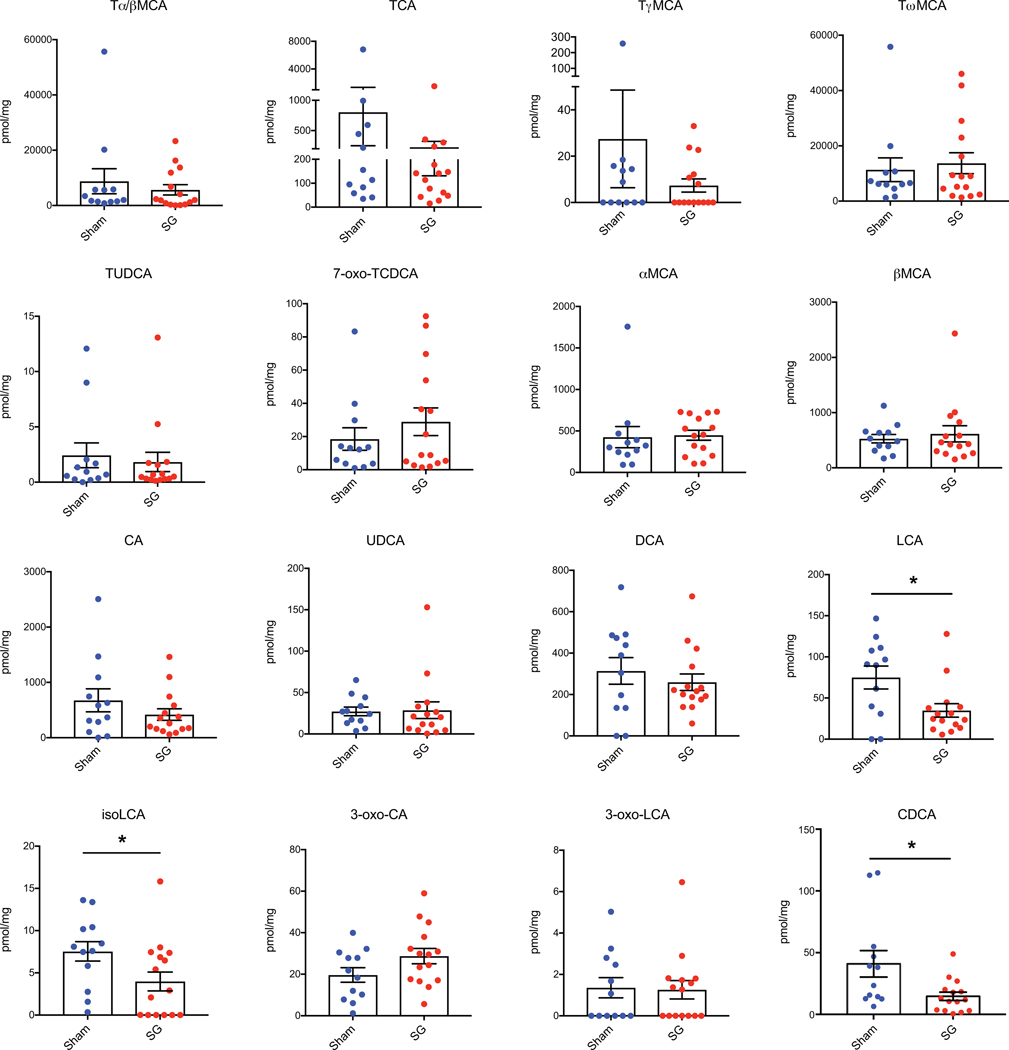
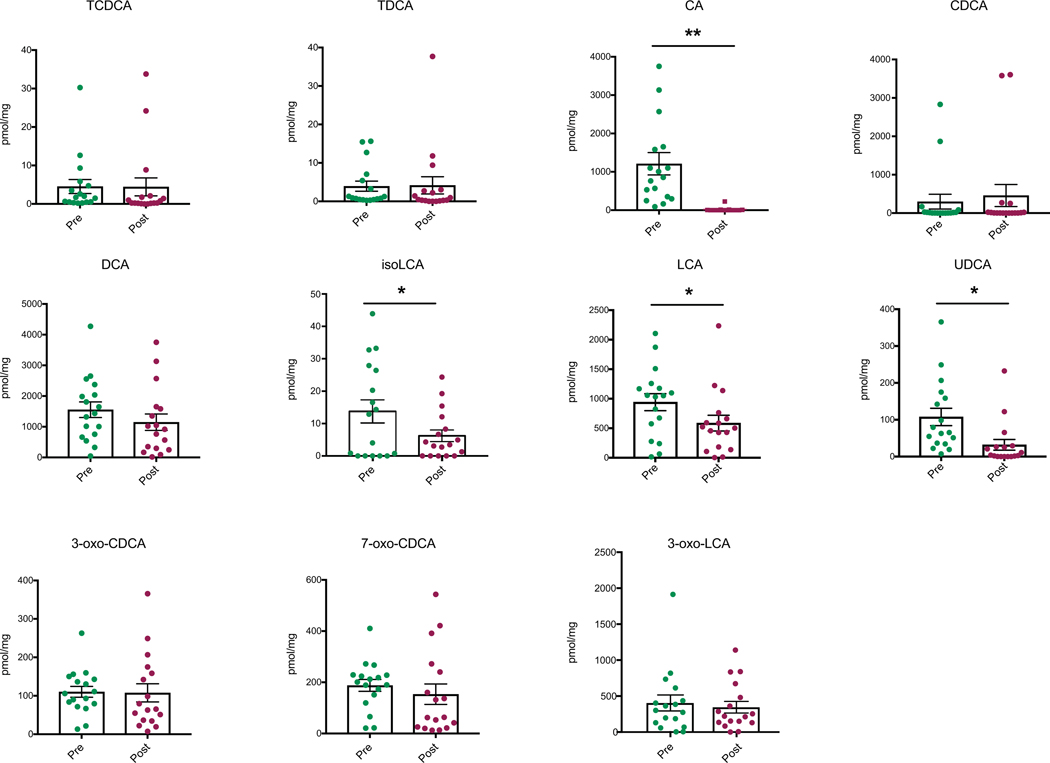
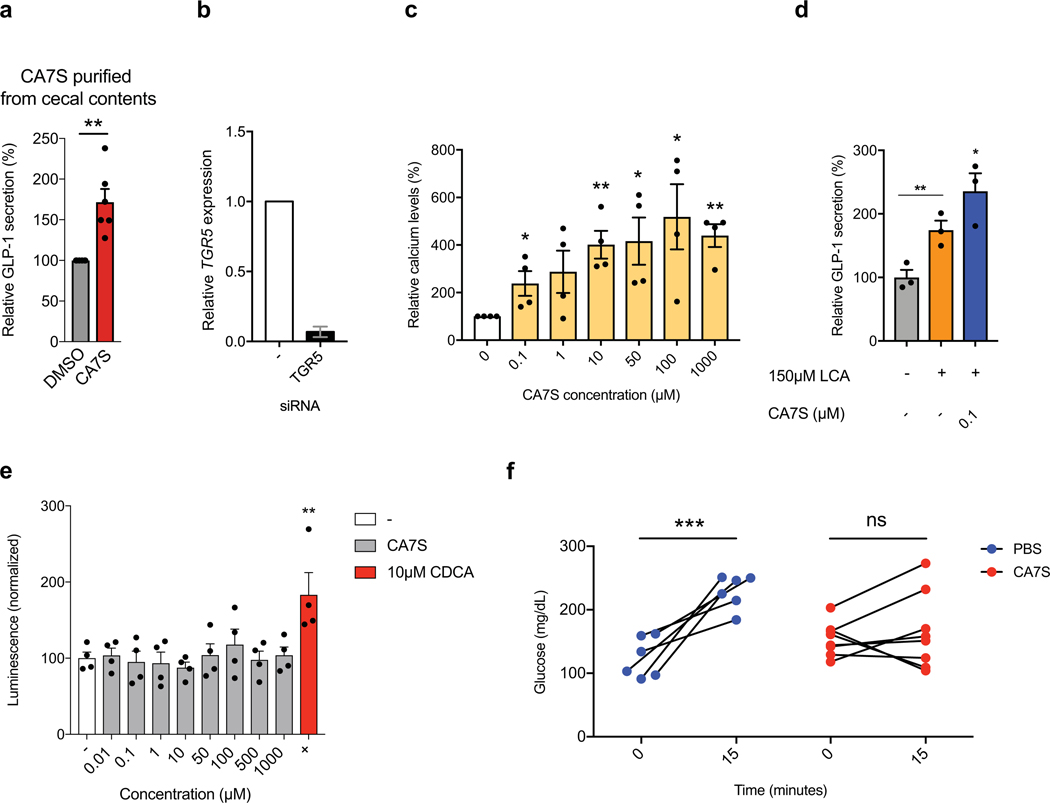
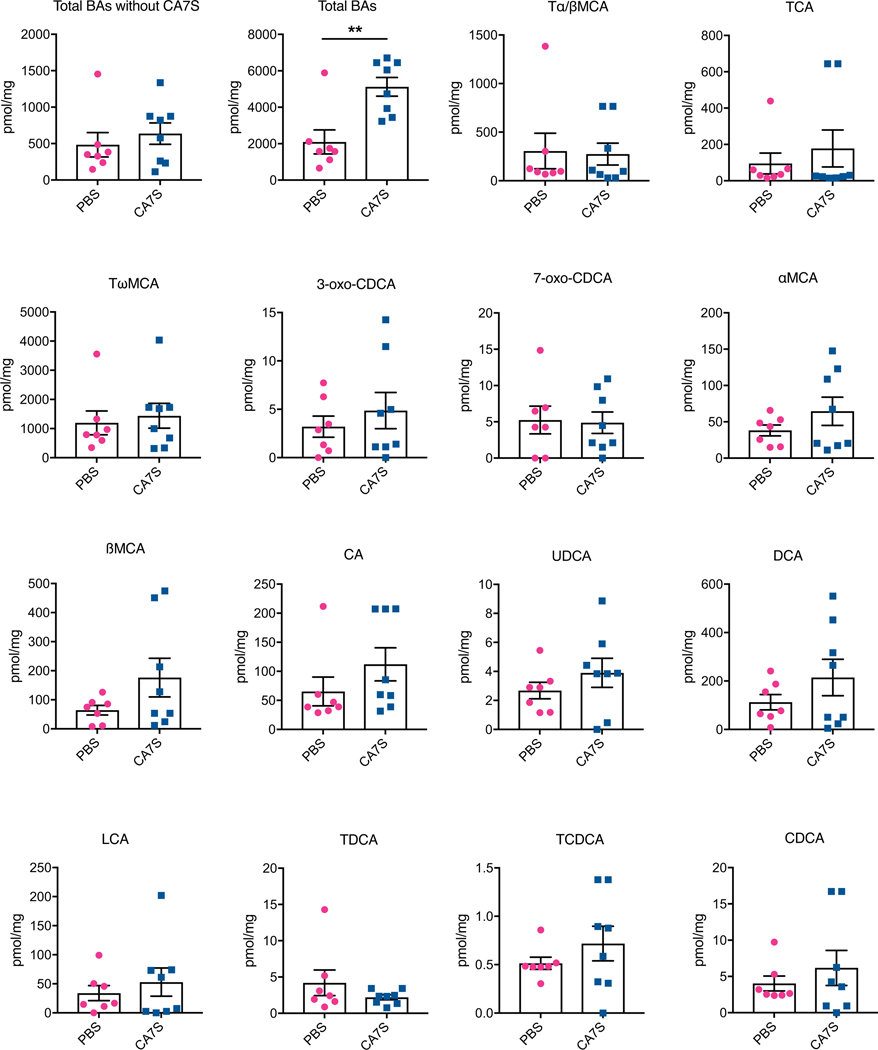
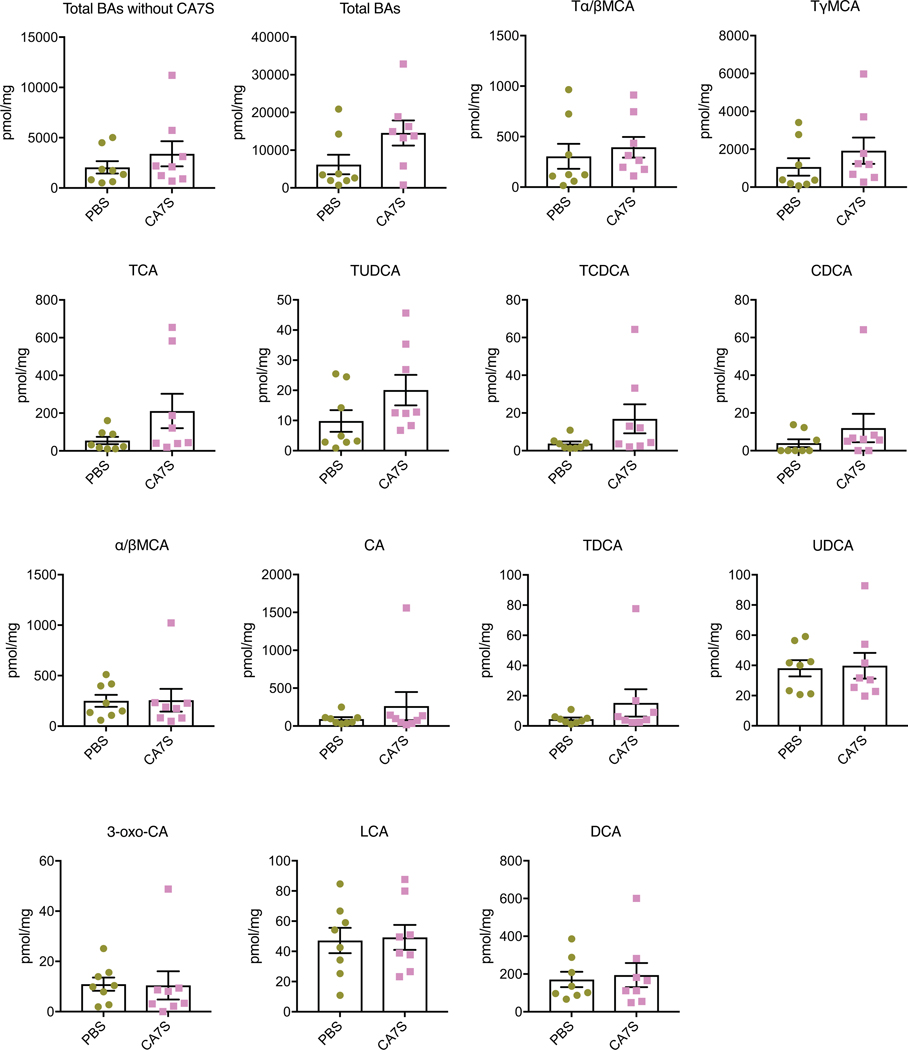
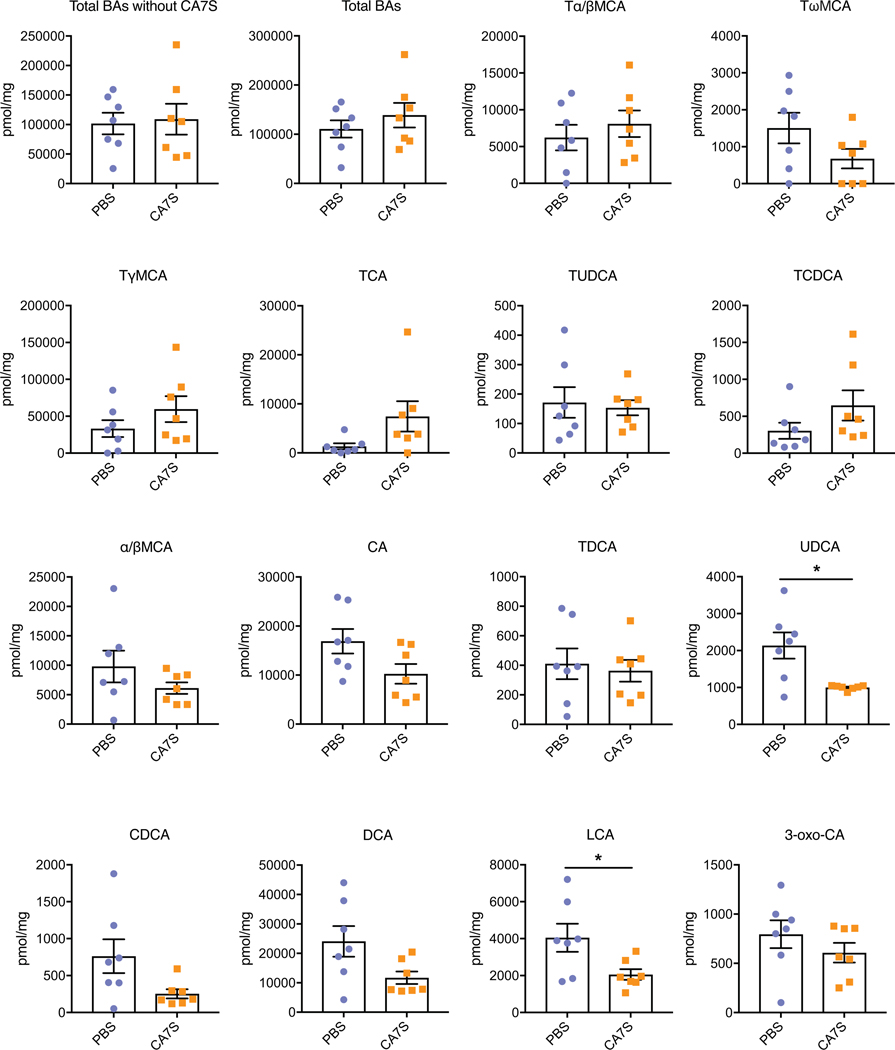
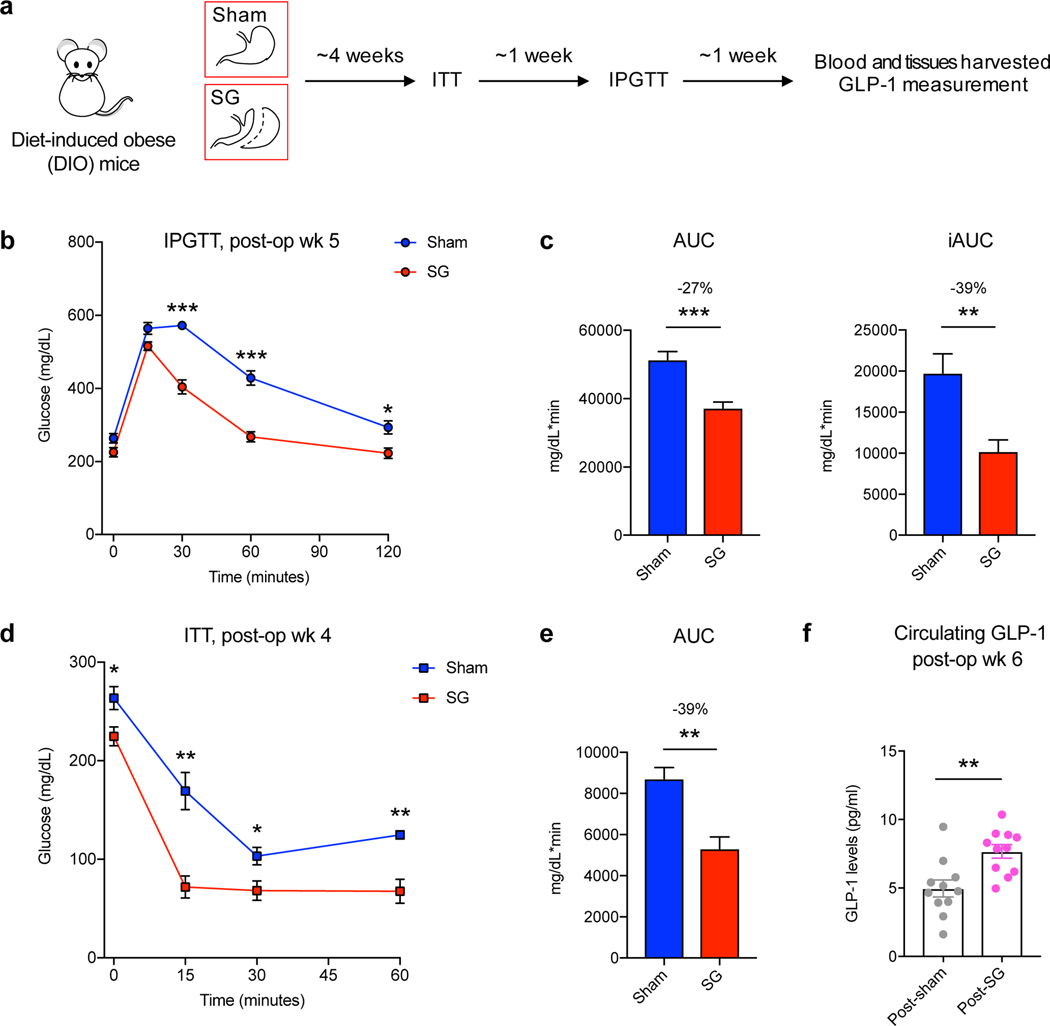
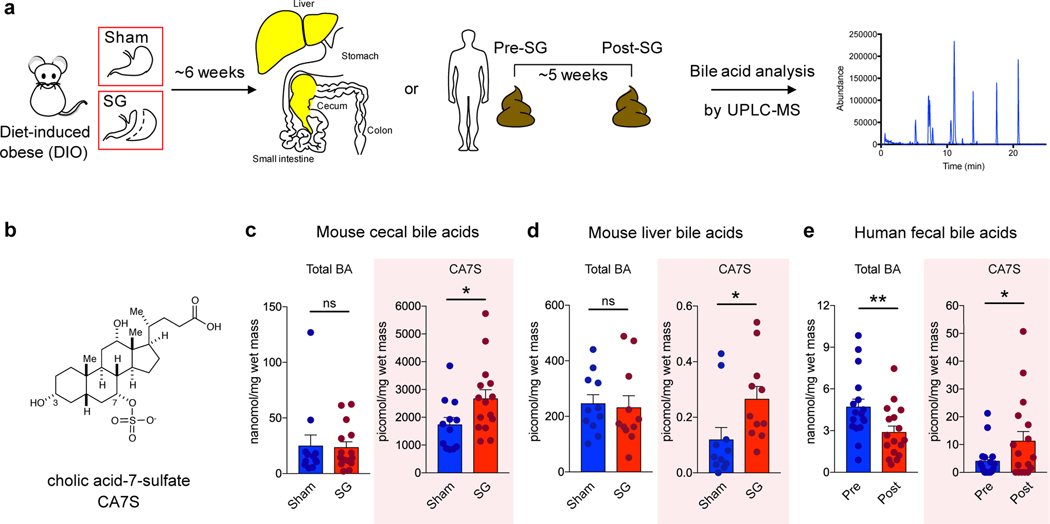
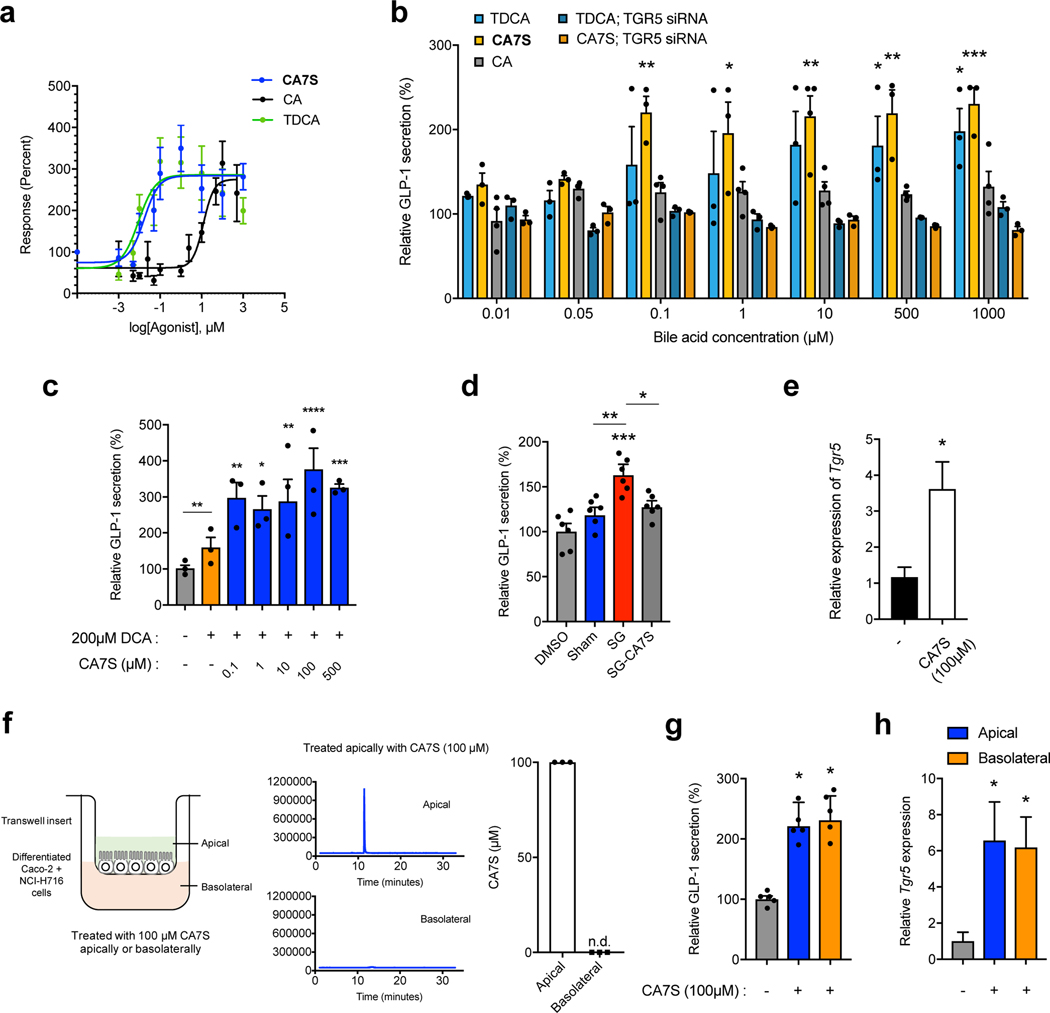
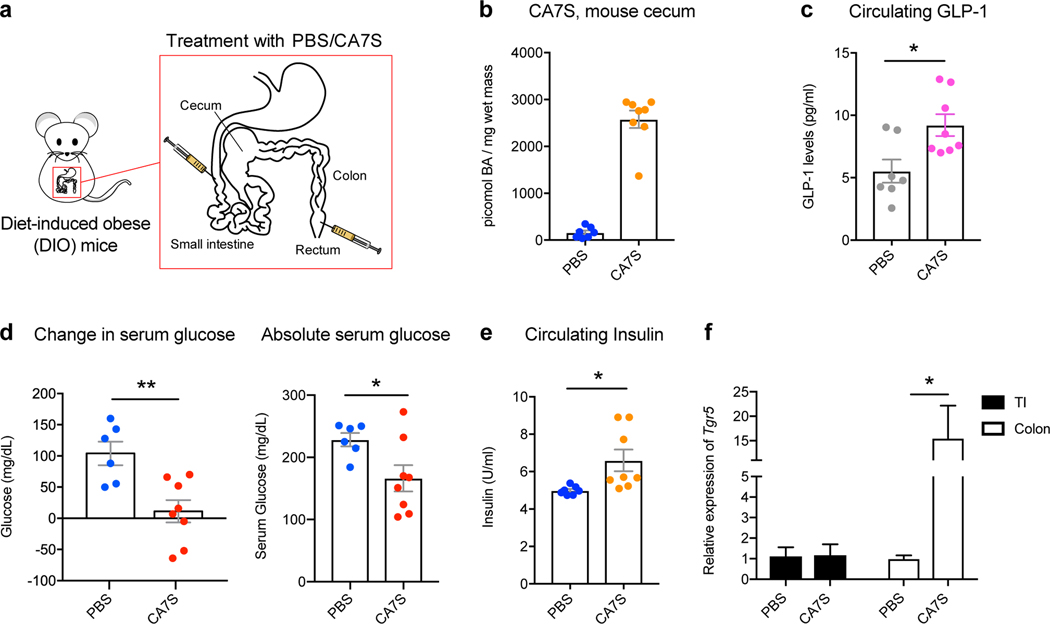
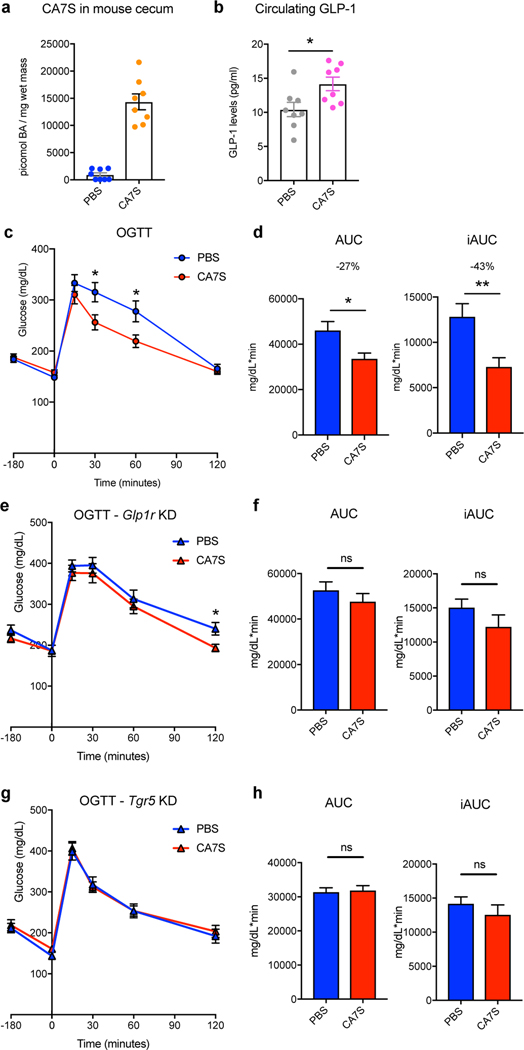
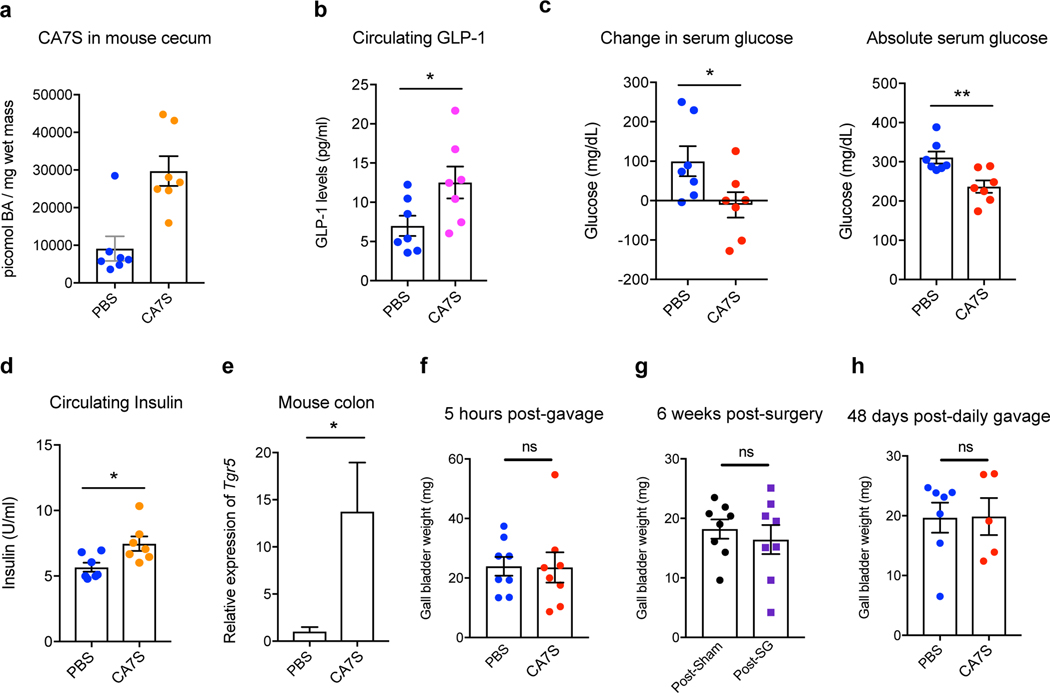
Bariatric surgery, the most effective treatment for obesity and type 2 diabetes, is associated with increased levels of the incretin hormone glucagon-like peptide-1 (GLP-1) and changes in levels of circulating bile acids. The levels of individual bile acids in the gastrointestinal (GI) tract after surgery have, however, remained largely unstudied. Using ultra-high performance liquid chromatography-mass spectrometry-based quantification, we observed an increase in an endogenous bile acid, cholic acid-7-sulfate (CA7S), in the GI tract of both mice and humans after sleeve gastrectomy. We show that CA7S is a Takeda G-protein receptor 5 (TGR5) agonist that increases Tgr5 expression and induces GLP-1 secretion. Furthermore, CA7S administration increases glucose tolerance in insulin-resistant mice in a TGR5-dependent manner. CA7S remains gut restricted, minimizing off-target effects previously observed for TGR5 agonists absorbed into the circulation. By studying changes in individual metabolites after surgery, the present study has revealed a naturally occurring TGR5 agonist that exerts systemic glucoregulatory effects while remaining confined to the gut.
Conflict of interest statement
Competing interests
CA7S is a subject of patents held by HMS and BWH on which S.N.C., D.A.H., E.G.S., and A.S.D. are inventors. A.S.D. is a consultant for Kintai Therapeutics and HP Hood. E.G.S. was previously on the scientific advisory board of Kitotech, Inc.
Figures
Comment in
-
Bariatric surgery works through a novel bile acid.Nat Chem Biol. 2021 Jan;17(1):5-6. doi: 10.1038/s41589-020-0648-0. Nat Chem Biol. 2021. PMID: 32848213 No abstract available.
References
Methods-only References
-
- Cristina ML, Lehy T, Zeitoun P. & Dufougeray F. Fine structural classification and comparative distribution of endocrine cells in normal human large intestine. Gastroenterology 75, 20–28 (1978). - PubMed
-
- Verhoeckx K. et al. Caco-2 Cell Line. The Impact of Food Bioactives on Health 175, 103–111 (2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
