

Accuracy of the clinical pulmonary infection score to differentiate ventilator-associated tracheobronchitis from ventilator-associated pneumonia
- PMID: 32748025
- PMCID: PMC7396887
- DOI: 10.1186/s13613-020-00721-4
Accuracy of the clinical pulmonary infection score to differentiate ventilator-associated tracheobronchitis from ventilator-associated pneumonia
Abstract
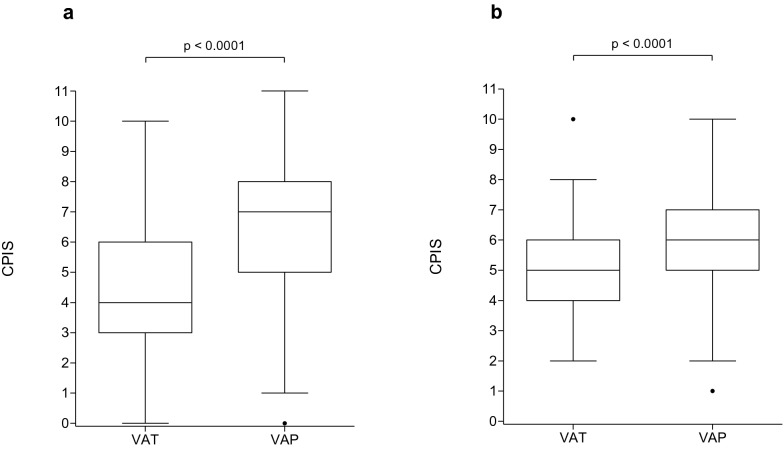
Background: Differentiating Ventilator-Associated Tracheobronchitis (VAT) from Ventilator-Associated Pneumonia (VAP) may be challenging for clinicians, yet their management currently differs. In this study, we evaluated the accuracy of the Clinical Pulmonary Infection Score (CPIS) to differentiate VAT and VAP.
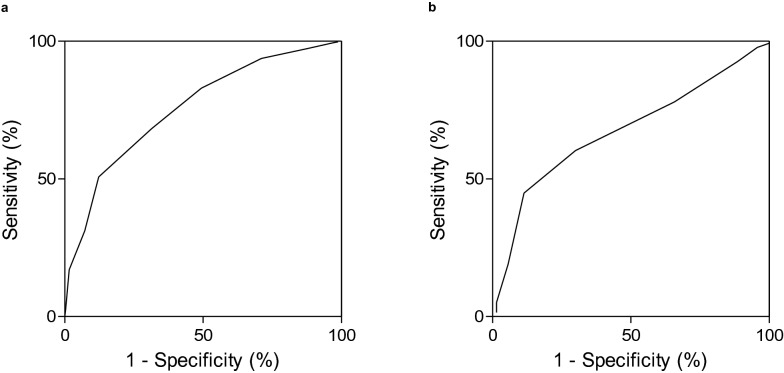
Methods: We performed a retrospective analysis based on the data from 2 independent prospective cohorts. Patients of the TAVeM database with a diagnosis of VAT (n = 320) or VAP (n = 369) were included in the derivation cohort. Patients admitted to the Intensive Care Centre of Lille University Hospital between January 1, 2016 and December 31, 2017 who had a diagnosis of VAT (n = 70) or VAP (n = 139) were included in the validation cohort. The accuracy of the CPIS to differentiate VAT from VAP was assessed within the 2 cohorts by calculating sensitivity and specificity values, establishing the ROC curves and choosing the best threshold according to the Youden index.
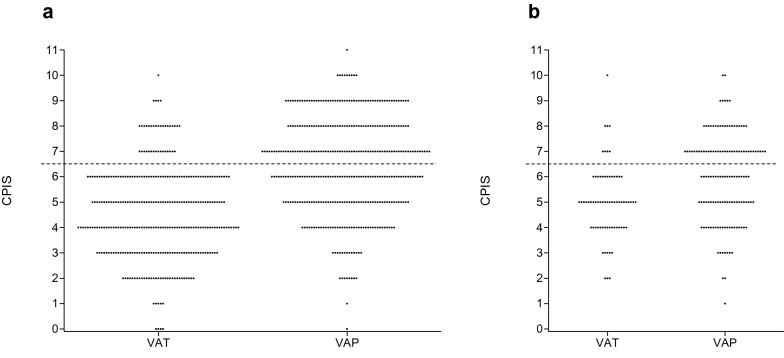
Results: The areas under ROC curves of CPIS to differentiate VAT from VAP were calculated at 0.76 (95% CI [0.72-0.79]) in the derivation cohort and 0.67 (95% CI [0.6-0.75]) in the validation cohort. A CPIS value ≥ 7 was associated with the highest Youden index in both cohorts. With this cut-off, sensitivity and specificity were respectively found at 0.51 and 0.88 in the derivation cohort, and at 0.45 and 0.89 in the validation cohort.
Conclusions: A CPIS value ≥ 7 reproducibly allowed to differentiate VAT from VAP with high specificity and PPV and moderate sensitivity and NPV in our derivation and validation cohorts.
Keywords: CPIS; Lower respiratory tract infection; Mechanical ventilation; Pneumonia; Tracheobronchitis.
Conflict of interest statement
SN reports personal fees from MSD, Pfizer, Gilead, Bio Rad, and Biomerieux, outside the submitted work; other authors have no competing interest to disclose. The authors declare that they have no competing interests.
Figures
References
-
- Torres A, Niederman MS, Chastre J, Ewig S, Fernandez-Vandellos P, Hanberger H, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017;50. - PubMed
-
- Butler KL, Sinclair KE, Henderson VJ, McKinney G, Mesidor DA, KatonBenitez I, et al. The chest radiograph in critically ill surgical patients is inaccurate in predicting ventilator-associated pneumonia. Am Surg. 1999;65:805–809. - PubMed
LinkOut - more resources
Full Text Sources
