

Extremely rare case of H-type gallbladder duplication coexistent with carcinoma: a case report and review of the literature
- PMID: 32748059
- PMCID: PMC7399013
- DOI: 10.1186/s40792-020-00953-3
Extremely rare case of H-type gallbladder duplication coexistent with carcinoma: a case report and review of the literature
Abstract
Introduction: Multiple gallbladders represent a rare congenital disorder, and coexistence with carcinoma is extremely rare, leading to a high possibility of misdiagnosis and surgical complications. In this study, a case was reported and the literature was reviewed.
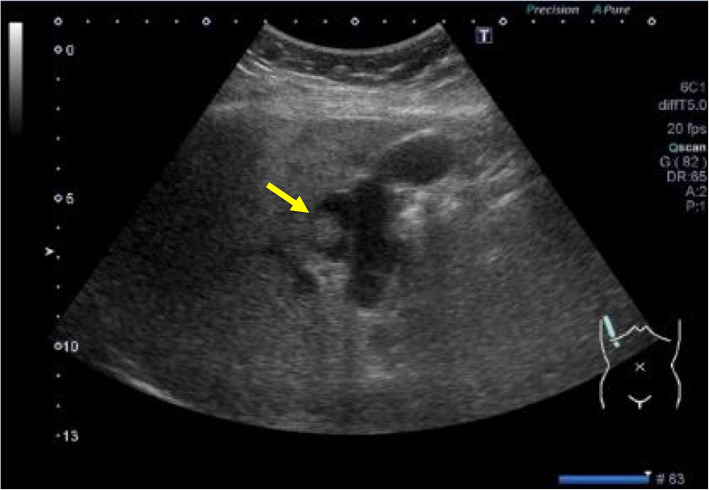
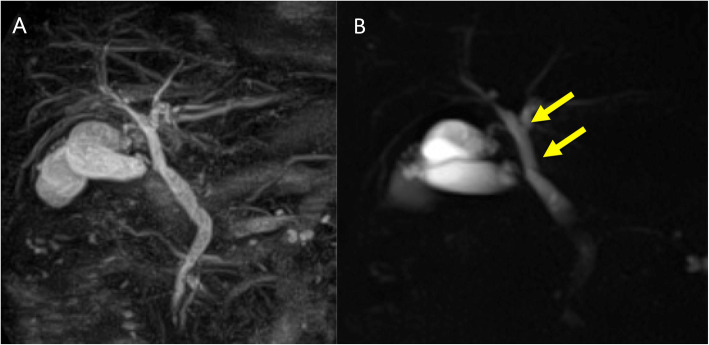
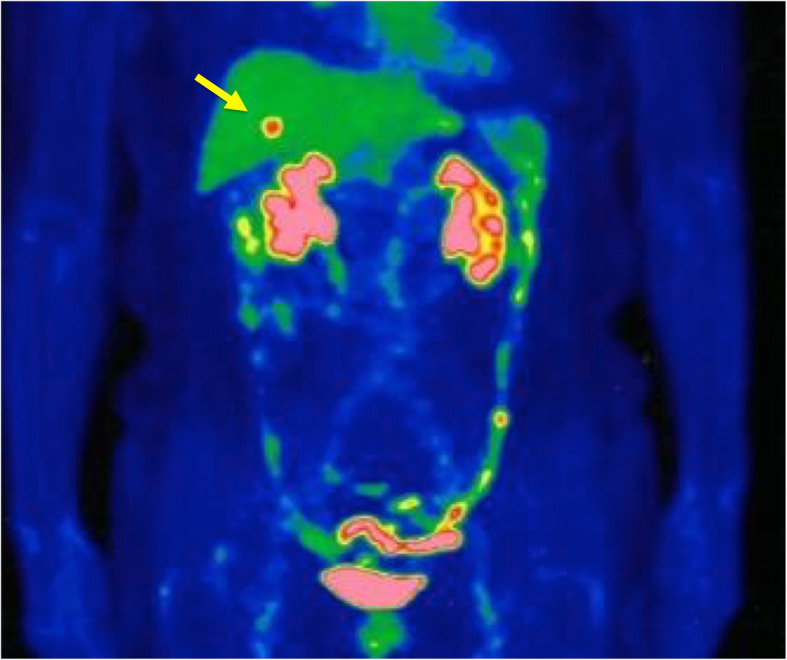
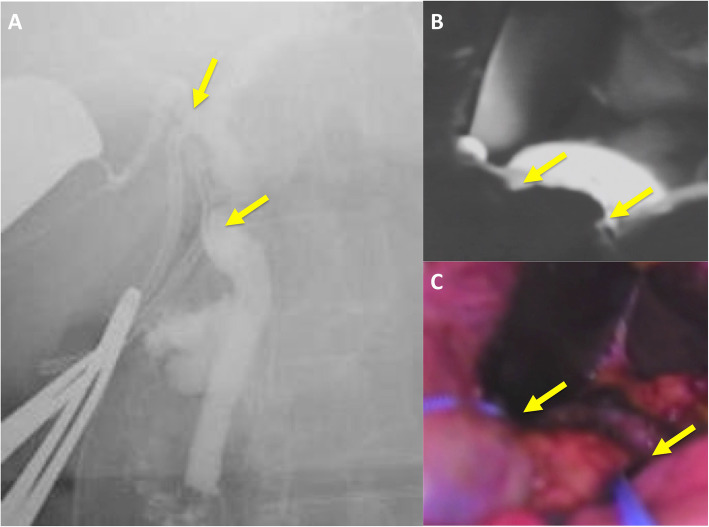
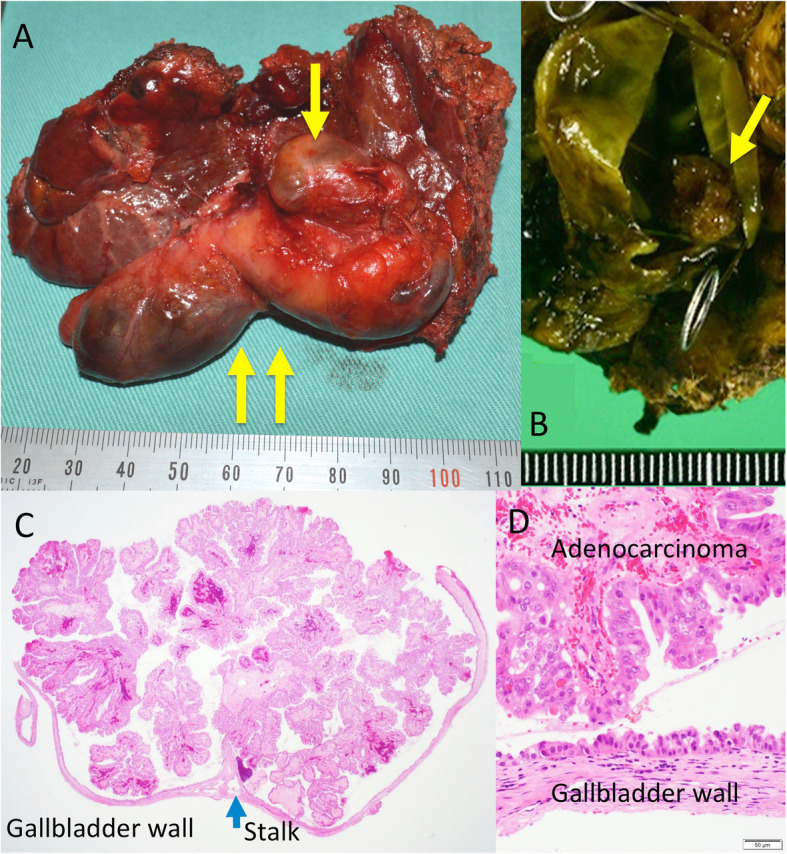
Case presentation: An 80-year-old woman was diagnosed with acute cholecystitis via ultrasonography and was successfully treated with antibiotics. After the patient's biliary colic relapsed, she was referred to our hospital. Multiple imaging modalities revealed duplication of her gallbladder (H-type) and suggested coexistence with carcinoma. According to preoperative evaluations, we assumed the patient had stage IIIA disease, and cholecystectomy, cholangiography using a near-infrared ray vision system, and sectionectomy of segments 4a and 5 were performed. Contrary to the high standardized uptake values obtained by 18F-fluoro-2-deoxy-D-glucose positron emission tomography, gallbladder carcinoma was pathologically diagnosed as stage 0 mucosal cancer. Seven days after the operation, portal thrombosis of the posterior branch was revealed, and conservative therapy was indicated; satisfactory results were achieved. The patient was discharged 65 days after surgery. No recurrence was observed for 1 year after surgery.
Conclusions: An extremely rare case of malignancy in a duplicated gallbladder was reported, and the literature was reviewed. Accurate estimations are feasible for diagnoses of multiple gallbladders, where correct evaluations are vital, especially in malignant cases. Because of the possibility of malignancy, resected accessory gallbladders should be scrutinized pathologically.
Keywords: Adenocarcinoma; FDG-PET; Gallbladder duplication; Intraoperative cholangiography; Near-infrared ray vision system.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Boyden EA. The accessory gallbladder-an embryological and comparative study of aberrant biliary vesicles occurring in man and domestic mammals. Am J Anast. 1926;38:177–231. doi: 10.1002/aja.1000380202. - DOI
-
- Raymond SW, Thrift CB. Carcinoma of a duplicated gallbladder. Illinois Med J. 1956;110:239–240. - PubMed
-
- Kin Y, Yamaguchi A, Isogai M, Hori A. Duplication of the gallbladder with advanced adenocarcinoma: diagnostic value of MRI and angiography. Hepatogastroenterology. 1996;43:405–408. - PubMed
LinkOut - more resources
Full Text Sources
