

Mechanisms and Rationale for Targeted Therapies in Refractory and Unexplained Chronic Cough
- PMID: 32748976
- PMCID: PMC7983941
- DOI: 10.1002/cpt.2003
Mechanisms and Rationale for Targeted Therapies in Refractory and Unexplained Chronic Cough
Abstract
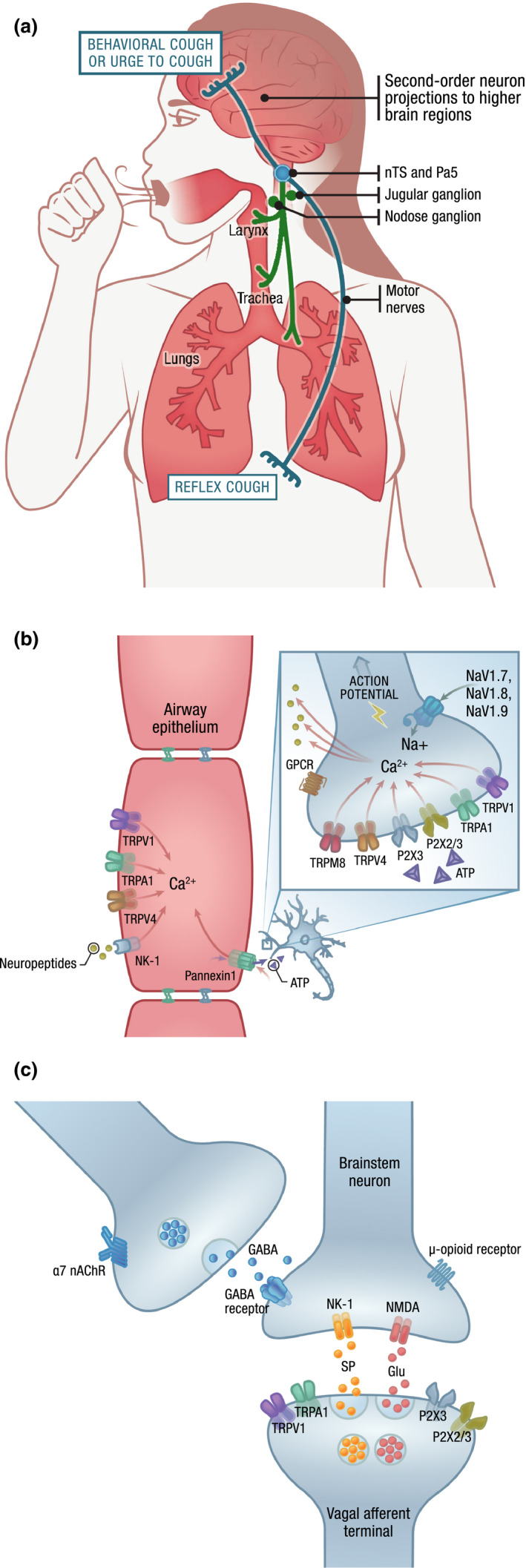
Chronic cough, defined as a cough lasting > 8 weeks, is a common medical condition that exerts a substantial physical, mental, and social burden on patients. A subset of patients with chronic cough are troubled with a cough that persists despite optimal treatment of presumed associated common and uncommon conditions (refractory chronic cough; RCC) or in which no diagnosable cause for cough can be identified despite extensive assessment (unexplained chronic cough; UCC). Many of these patients exhibit clinical features of cough hypersensitivity, including laryngeal paresthesia, hypertussia, and allotussia. Over-the-counter cough remedies are ineffective and can lead to intolerable side effects when used for RCC/UCC, and the lack of approved treatments indicated for these conditions reflects a major unmet need. An increased understanding of the anatomy and neurophysiology of protective and pathologic cough has fostered a robust clinical development pipeline of several targeted therapies for RCC/UCC. This manuscript reviews the mechanisms presumed to underly RCC/UCC together with the rationale and clinical evidence for several targeted therapies currently under clinical investigation, including transient receptor potential channel antagonists, P2X3-receptor antagonists, voltage-gated sodium channel blockers, neuromodulators, and neurokinin-1-receptor antagonists. Finally, we provide an overview of targets that have been investigated in preclinical models of cough and other airway diseases that may hold future promise for clinical studies in RCC/UCC. Development of targeted therapies with different sites of action may foster a precision medicine approach to treat this heterogeneous, underserved patient population.
© 2020 The Authors. Clinical Pharmacology & Therapeutics published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
S.M. declares personal fees from Merck and NeRRe Therapeutics and grant support from Merck. L.M. reports personal fees from Chiesi, GSK, Merck, NeRRe Therapeutics, and Shionogi Inc; grant support from Merck; and other support from AstraZeneca, Boehringer Ingelheim, and Chiesi.
Figures
References
-
- Song, W.J. et al. The global epidemiology of chronic cough in adults: a systematic review and meta‐analysis. Eur. Respir. J. 45, 1479–1481 (2015). - PubMed
-
- French, C.L. , Crawford, S.L. , Bova, C. & Irwin, R.S. Change in psychological, physiological, and situational factors in adults after treatment of chronic cough. Chest 152, 547–562 (2017). - PubMed
-
- Chamberlain, S.A.F. et al. The impact of chronic cough: a cross‐sectional European survey. Lung 193, 401–408 (2015). - PubMed
-
- Kuzniar, T.J. , Morgenthaler, T.I. , Afessa, B. & Lim, K.G. Chronic cough from the patient's perspective. Mayo. Clin. Proc. 82, 56–60 (2007). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
