

ADNC-RS, a clinical-genetic risk score, predicts Alzheimer's pathology in autopsy-confirmed Parkinson's disease and Dementia with Lewy bodies
- PMID: 32749525
- PMCID: PMC7864557
- DOI: 10.1007/s00401-020-02199-7
ADNC-RS, a clinical-genetic risk score, predicts Alzheimer's pathology in autopsy-confirmed Parkinson's disease and Dementia with Lewy bodies
Abstract
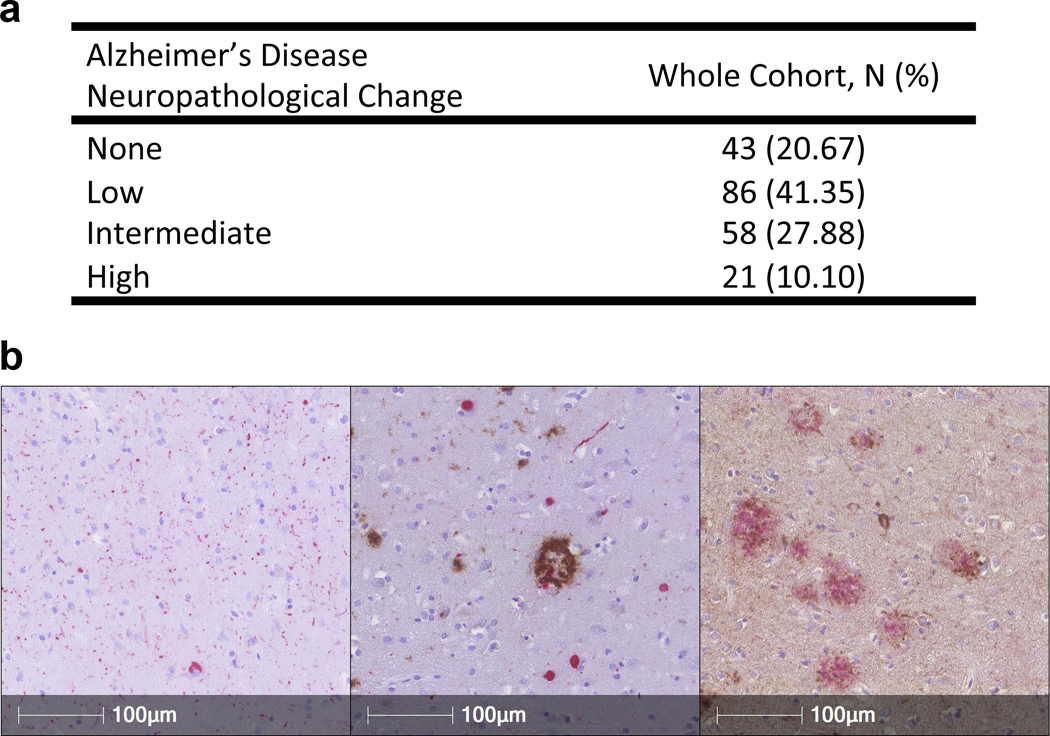
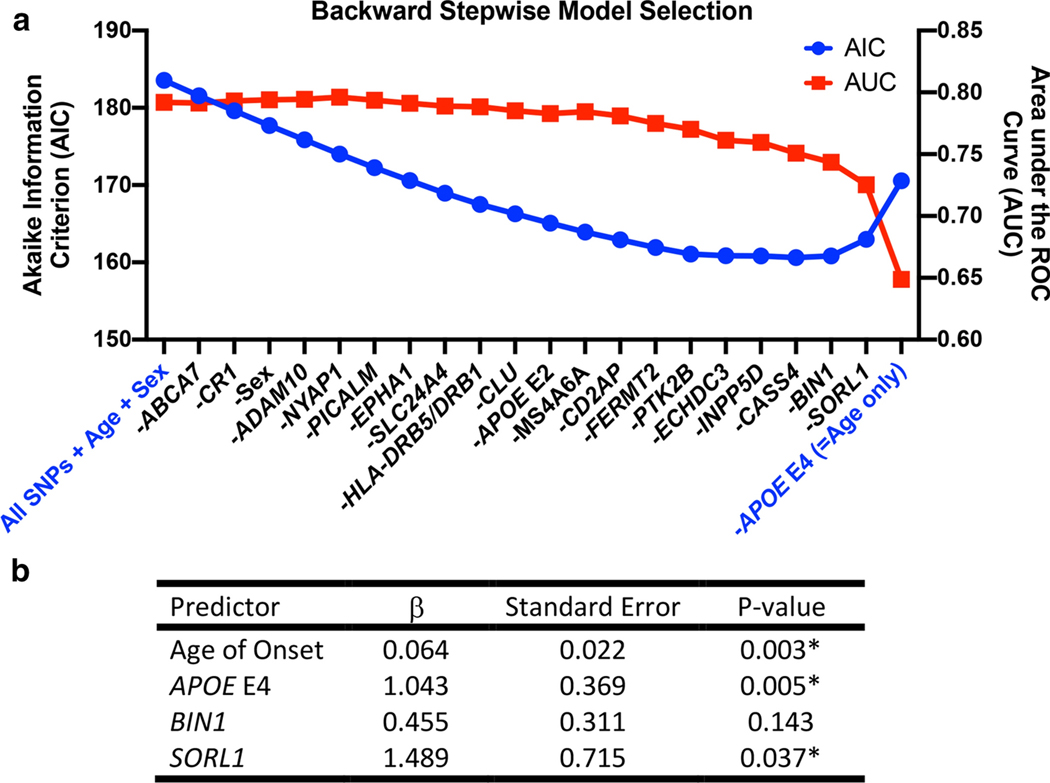
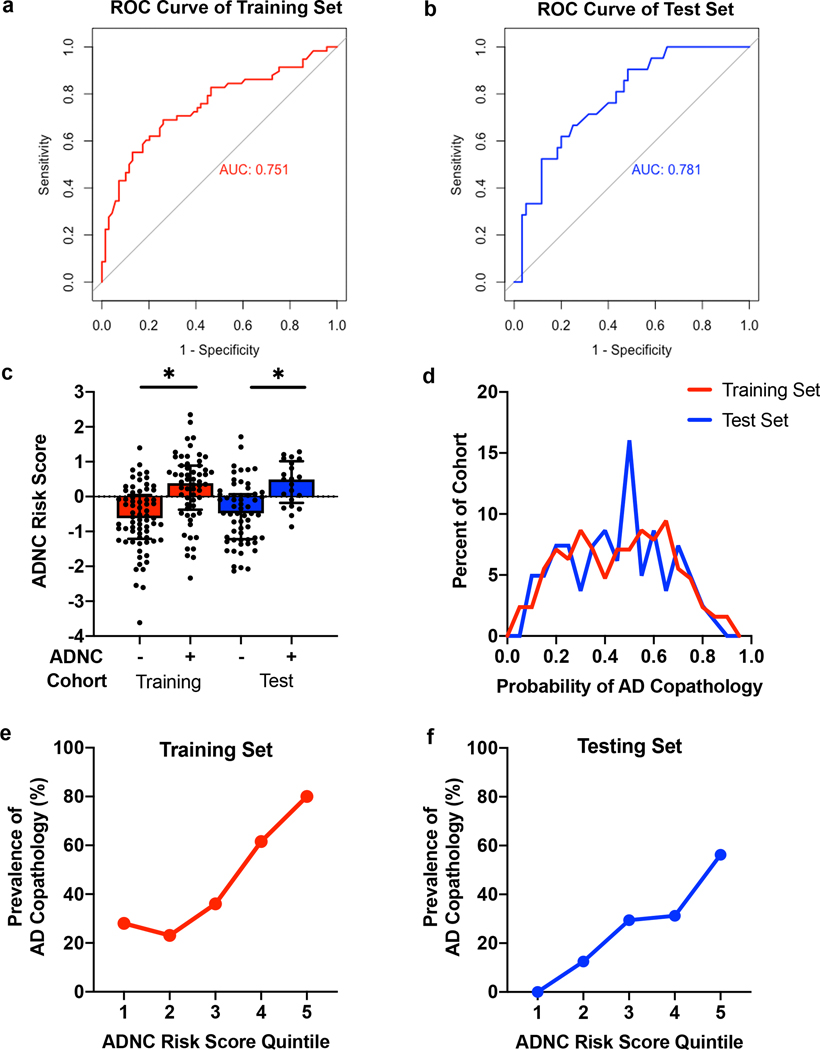
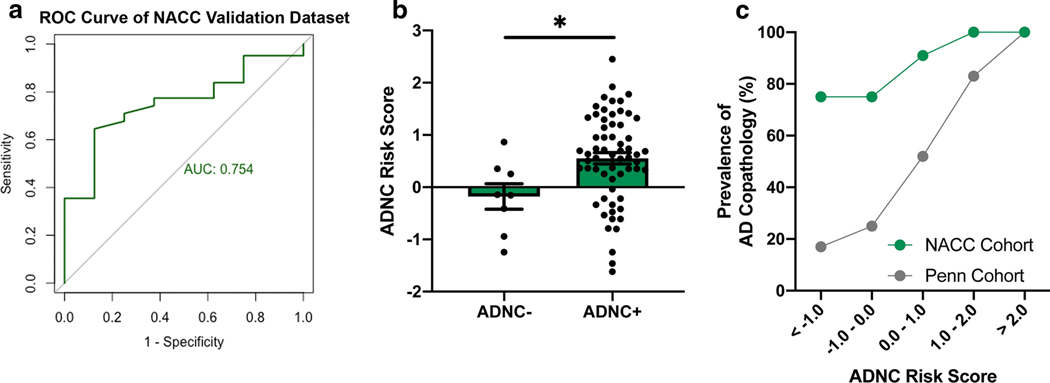
Growing evidence suggests overlap between Alzheimer's disease (AD) and Parkinson's disease (PD) pathophysiology in a subset of patients. Indeed, 50-80% of autopsy cases with a primary clinicopathological diagnosis of Lewy body disease (LBD)-most commonly manifesting during life as PD-have concomitant amyloid-beta and tau pathology, the defining pathologies of AD. Here we evaluated common genetic variants in genome-wide association with AD as predictors of concomitant AD pathology in the brains of people with a primary clinicopathological diagnosis of PD or Dementia with Lewy Bodies (DLB), diseases both characterized by neuronal Lewy bodies. In the first stage of our study, 127 consecutive autopsy-confirmed cases of PD or DLB from a single center were assessed for AD neuropathological change (ADNC), and these same cases were genotyped at 20 single nucleotide polymorphisms (SNPs) found by genome-wide association study to associate with risk for AD. In these 127 training set individuals, we developed a logistic regression model predicting the presence of ADNC, using backward stepwise regression for model selection and tenfold cross-validation to estimate performance. The best-fit model generated a risk score for ADNC (ADNC-RS) based on age at disease onset and genotype at three SNPs (APOE, BIN1, and SORL1 loci), with an area under the receiver operating curve (AUC) of 0.751 in our training set. In the replication stage of our study, we assessed model performance in a separate test set of the next 81 individuals genotyped in our center. In the test set, the AUC was 0.781, and individuals with ADNC-RS in the top quintile had four-fold increased likelihood of having AD pathology at autopsy compared with those in each of the lowest two quintiles. Finally, in the validation stage of our study, we applied our ADNC-RS model to 70 LBD individuals from 20 Alzheimer's Disease Research Centers (ADRC) whose autopsy and genetic data were available in the National Alzheimer's Coordinating Center (NACC) database. In this validation set, the AUC was 0.754. Thus, in patients with autopsy-confirmed PD or DLB, a simple model incorporating three AD-risk SNPs and age at disease onset substantially enriches for concomitant AD pathology at autopsy, with implications for identifying LBD patients in which targeting amyloid-beta or tau is a therapeutic strategy.
Keywords: Alzheimer’s disease; Dementia; Genetics; Parkinson’s disease.
Figures
References
-
- Beekly DL, Ramos EM, Van Belle G, Deitrich W, Clark AD, Jacka ME, et al. (2004) The National Alzheimer’ s Coordinating Center (NACC) Database: An Alzheimer Disease Database. Alzheimer Dis Assoc Disord 18:270–277 - PubMed
Publication types
MeSH terms
Grants and funding
- RC2 AG036528/AG/NIA NIH HHS/United States
- P50 AG005142/AG/NIA NIH HHS/United States
- P50 AG005146/AG/NIA NIH HHS/United States
- U01 AG032984/AG/NIA NIH HHS/United States
- T32 GM007170/GM/NIGMS NIH HHS/United States
- P50 AG047266/AG/NIA NIH HHS/United States
- P30 AG008017/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- P50 AG025688/AG/NIA NIH HHS/United States
- P30 AG010124/NS/NINDS NIH HHS/United States
- R01 NS115139/NS/NINDS NIH HHS/United States
- P50 AG005138/AG/NIA NIH HHS/United States
- P50 AG047366/AG/NIA NIH HHS/United States
- P30 AG019610/AG/NIA NIH HHS/United States
- P30 AG028383/AG/NIA NIH HHS/United States
- P30 AG013854/AG/NIA NIH HHS/United States
- P30 AG053760/AG/NIA NIH HHS/United States
- R01 NS082265/NS/NINDS NIH HHS/United States
- K23 NS114167/NS/NINDS NIH HHS/United States
- P30 AG062428/AG/NIA NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
- U24 AG021886/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- T32 AG000255/AG/NIA NIH HHS/United States
- P30 AG035982/AG/NIA NIH HHS/United States
- P50 AG008702/AG/NIA NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- P30 AG008051/AG/NIA NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- P30 AG013846/AG/NIA NIH HHS/United States
- P50 AG047270/AG/NIA NIH HHS/United States
- P30 AG062429/AG/NIA NIH HHS/United States
- P50 AG005136/AG/NIA NIH HHS/United States
- P30 AG049638/AG/NIA NIH HHS/United States
- P30 AG012300/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P50 AG016573/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- P30 AG066509/AG/NIA NIH HHS/United States
- U19 AG062418/AG/NIA NIH HHS/United States
- U19 AG062418/NS/NINDS NIH HHS/United States
- P30 AG062715/AG/NIA NIH HHS/United States
- RO1 NS115139/NS/NINDS NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
