

Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: a series of 91 cases
- PMID: 32749530
- PMCID: PMC7399600
- DOI: 10.1007/s00247-020-04747-5
Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: a series of 91 cases
Abstract
Background: Pulmonary infection with SARS-CoV-2 virus (severe acute respiratory syndrome coronavirus 2; COVID-19) has rapidly spread worldwide to become a global pandemic.
Objective: To collect paediatric COVID-19 cases worldwide and to summarize both clinical and imaging findings in children who tested positive on polymerase chain reaction testing for SARS-CoV-2.
Materials and methods: Data were collected by completion of a standardised case report form submitted to the office of the European Society of Paediatric Radiology from March 12 to April 8, 2020. Chest imaging findings in children younger than 18 years old who tested positive on polymerase chain reaction testing for SARS-CoV-2 were included. Representative imaging studies were evaluated by multiple senior paediatric radiologists from this group with expertise in paediatric chest imaging.
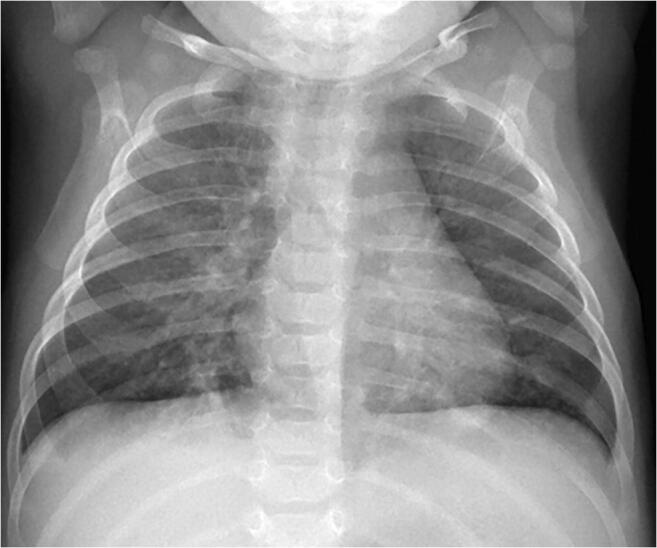
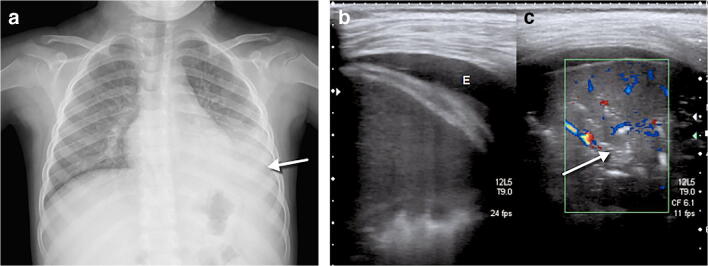
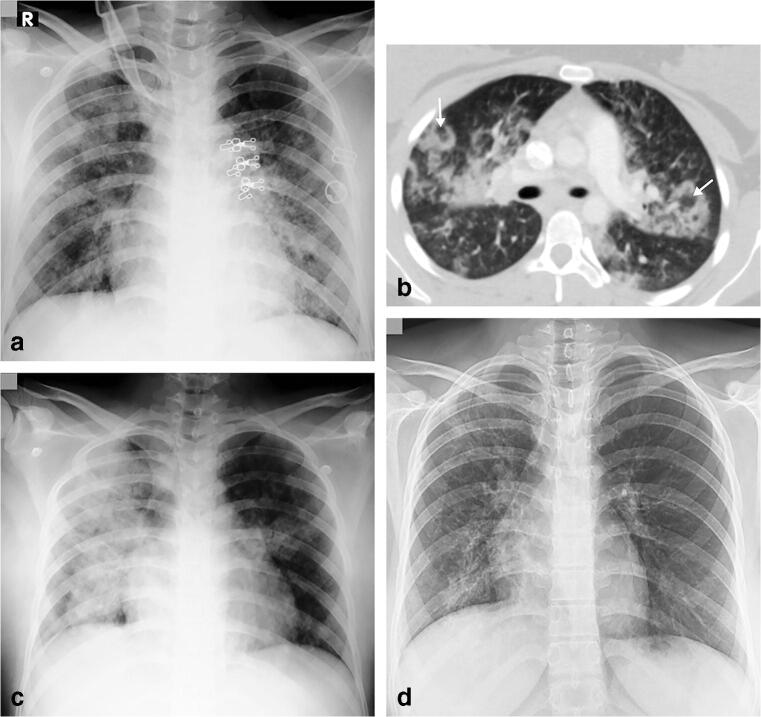
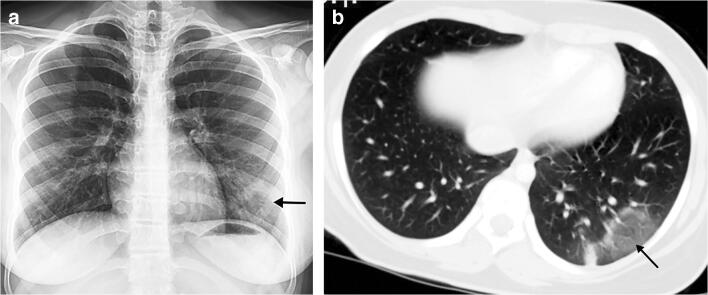
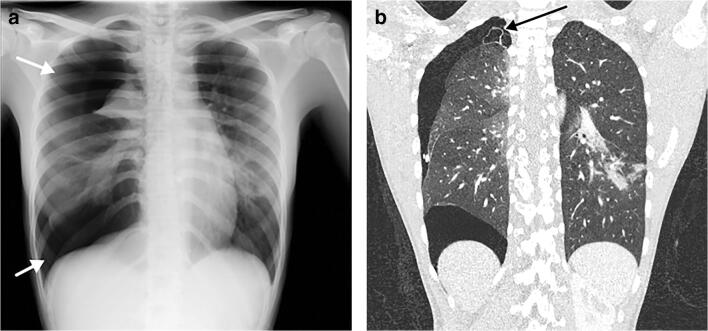
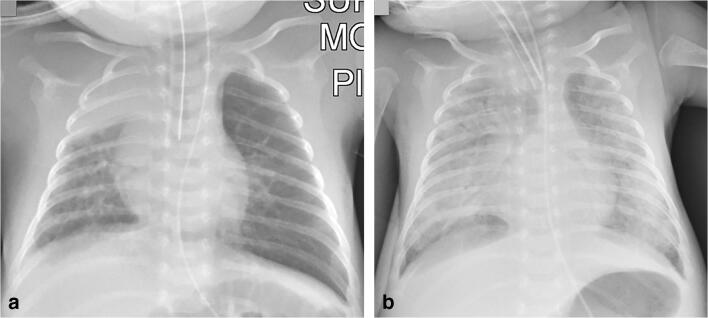
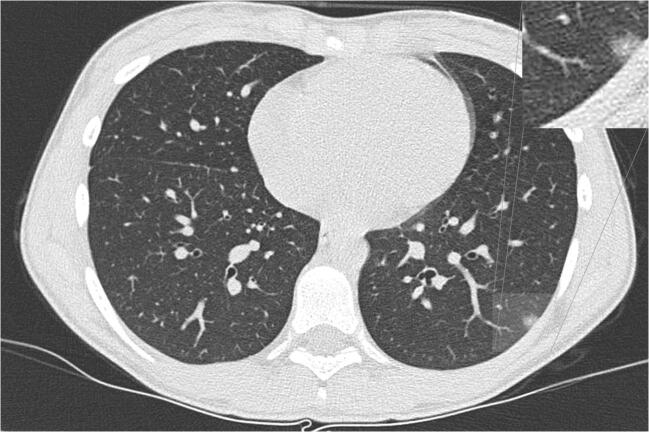
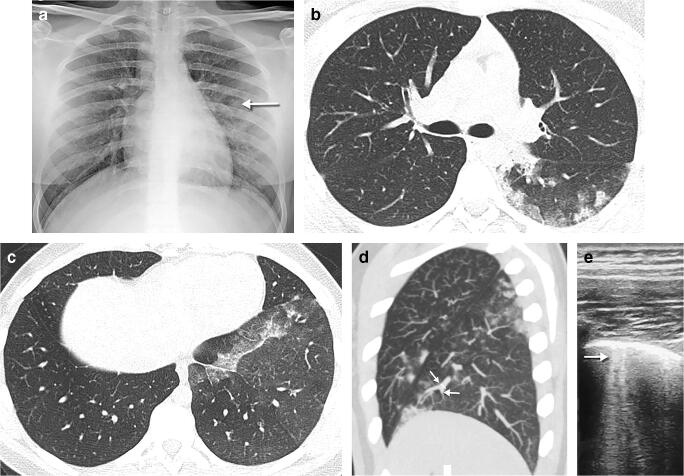
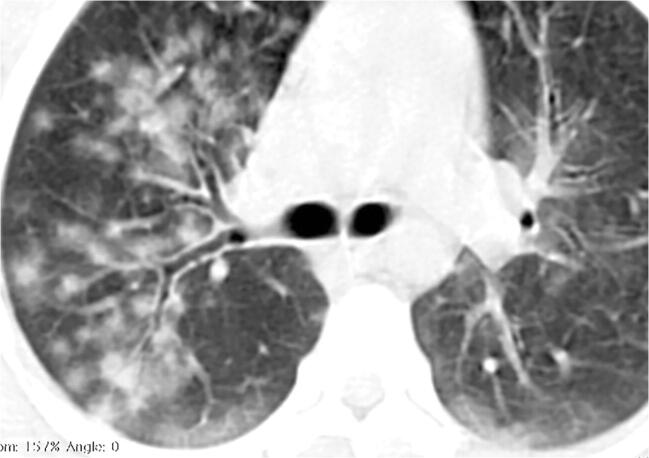
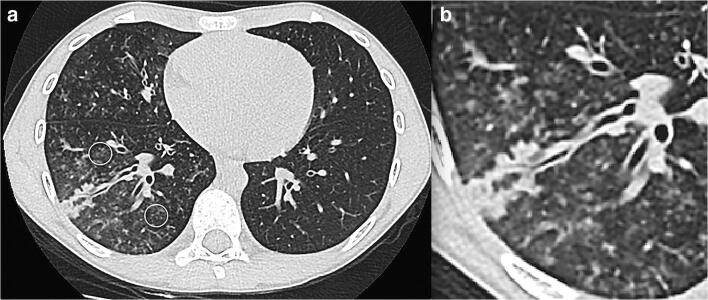
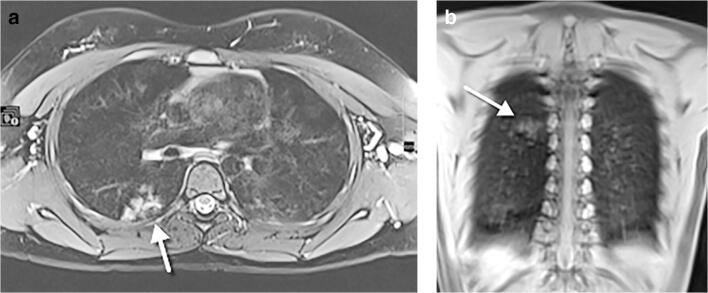
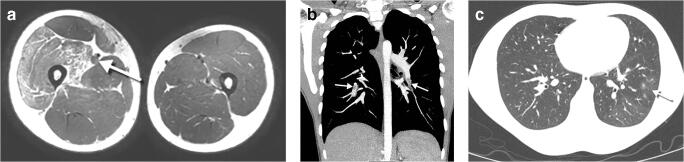
Results: Ninety-one children were included (49 males; median age: 6.1 years, interquartile range: 1.0 to 13.0 years, range: 9 days-17 years). Most had mild symptoms, mostly fever and cough, and one-third had coexisting medical conditions. Eleven percent of children presented with severe symptoms and required intensive unit care. Chest radiographs were available in 89% of patients and 10% of them were normal. Abnormal chest radiographs showed mainly perihilar bronchial wall thickening (58%) and/or airspace consolidation (35%). Computed tomography (CT) scans were available in 26% of cases, with the most common abnormality being ground glass opacities (88%) and/or airspace consolidation (58%). Tree in bud opacities were seen in 6 of 24 CTs (25%). Lung ultrasound and chest magnetic resonance imaging were rarely utilized.
Conclusion: It seems unnecessary to perform chest imaging in children to diagnose COVID-19. Chest radiography can be used in symptomatic children to assess airway infection or pneumonia. CT should be reserved for when there is clinical concern to assess for possible complications, especially in children with coexisting medical conditions.
Keywords: COVID-19; Children; Computed tomography; Coronavirus; Imaging; Lower respiratory tract infection; Pneumonitis; Radiography.
Figures





References
-
- Dong Y, Mo X, Hu Y et al (2020) Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 10.1542/peds.2020-0702
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
