

Best Practices for Chiropractic Management of Patients with Chronic Musculoskeletal Pain: A Clinical Practice Guideline
- PMID: 32749874
- PMCID: PMC7578188
- DOI: 10.1089/acm.2020.0181
Best Practices for Chiropractic Management of Patients with Chronic Musculoskeletal Pain: A Clinical Practice Guideline
Abstract
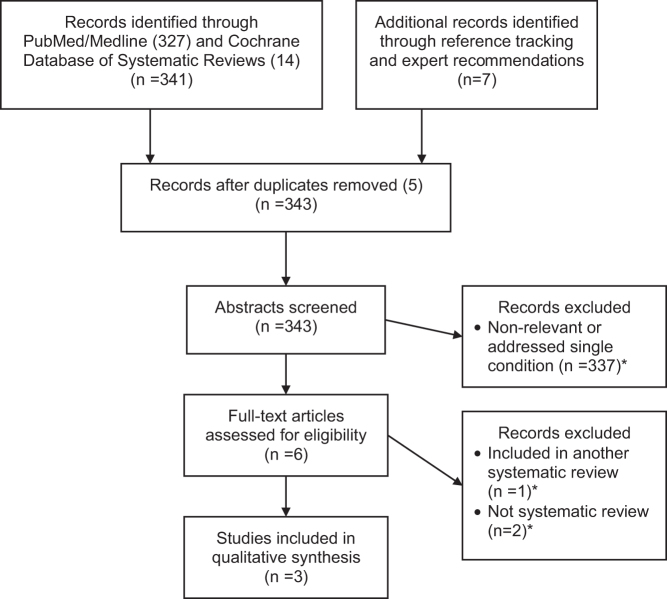
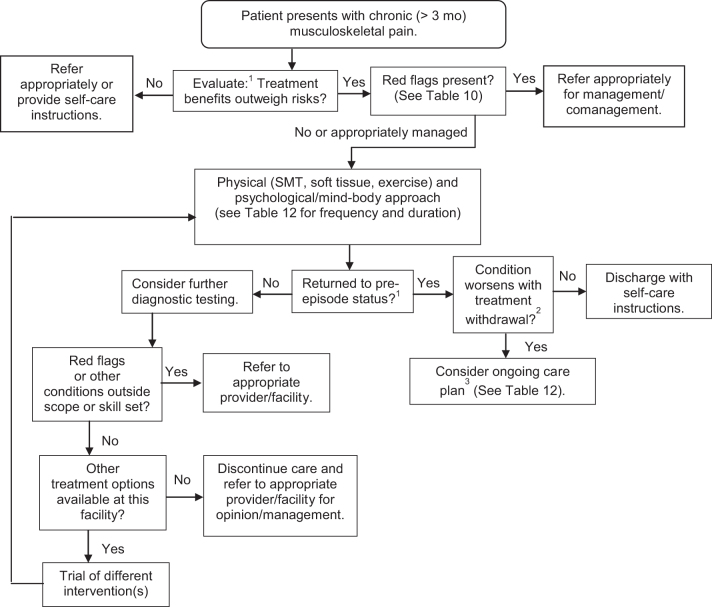
Objective: To develop an evidence-based clinical practice guideline (CPG) through a broad-based consensus process on best practices for chiropractic management of patients with chronic musculoskeletal (MSK) pain. Design: CPG based on evidence-based recommendations of a panel of experts in chronic MSK pain management. Methods: Using systematic reviews identified in an initial literature search, a steering committee of experts in research and management of patients with chronic MSK pain drafted a set of recommendations. Additional supportive literature was identified to supplement gaps in the evidence base. A multidisciplinary panel of experienced practitioners and educators rated the recommendations through a formal Delphi consensus process using the RAND Corporation/University of California, Los Angeles, methodology. Results: The Delphi process was conducted January-February 2020. The 62-member Delphi panel reached consensus on chiropractic management of five common chronic MSK pain conditions: low-back pain (LBP), neck pain, tension headache, osteoarthritis (knee and hip), and fibromyalgia. Recommendations were made for nonpharmacological treatments, including acupuncture, spinal manipulation/mobilization, and other manual therapy; modalities such as low-level laser and interferential current; exercise, including yoga; mind-body interventions, including mindfulness meditation and cognitive behavior therapy; and lifestyle modifications such as diet and tobacco cessation. Recommendations covered many aspects of the clinical encounter, from informed consent through diagnosis, assessment, treatment planning and implementation, and concurrent management and referral. Appropriate referral and comanagement were emphasized. Conclusions: These evidence-based recommendations for a variety of conservative treatment approaches to the management of common chronic MSK pain conditions may advance consistency of care, foster collaboration between provider groups, and thereby improve patient outcomes.
Keywords: chiropractic; chronic musculoskeletal pain; chronic pain; clinical practice guideline; spinal manipulation.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Nahin RL, Sayer B, Stussman BJ, Feinberg TM. Eighteen-year trends in the prevalence of, and health care use for, noncancer pain in the United States: Data from the Medical Expenditure Panel Survey. J Pain 2019;20:796–809 - PubMed
-
- Qaseem A, Wilt TJ, McLean RM, et al. . Noninvasive treatments for acute, subacute, and chronic low back pain: A clinical practice guideline from the American College of Physicians. Ann Intern Med 2017;166:514–530 - PubMed
-
- Clauw DJ, Essex MN, Pitman V, Jones KD. Reframing chronic pain as a disease, not a symptom: Rationale and implications for pain management. Postgrad Med 2019;131:185–198 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous