

Temporal Trends in Pregnancy-Associated Stroke and Its Outcomes Among Women With Hypertensive Disorders of Pregnancy
- PMID: 32750300
- PMCID: PMC7792242
- DOI: 10.1161/JAHA.120.016182
Temporal Trends in Pregnancy-Associated Stroke and Its Outcomes Among Women With Hypertensive Disorders of Pregnancy
Abstract
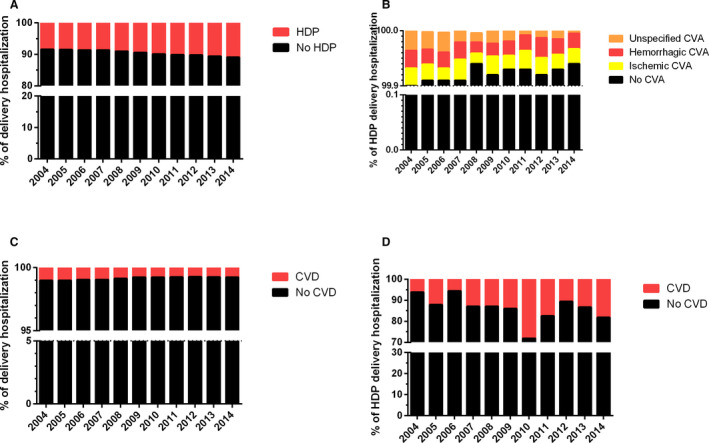
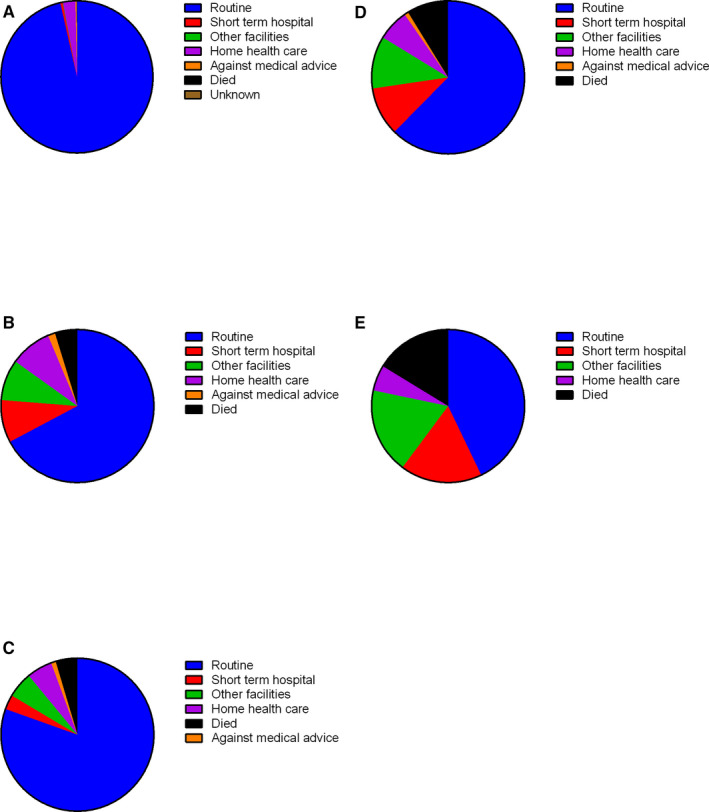
Background Stroke is a serious complication of hypertensive disorders of pregnancy (HDP), with potentially severe and long-term sequelae. However, the temporal trends, predictors, and outcomes of stroke in women with HDP at delivery remain unknown. Methods and Results All HDP delivery hospitalizations with or without stroke event (ischemic, hemorrhagic, or unspecified) between 2004 and 2014 in the United States National Inpatient Sample were analyzed to examine incidence, predictors, and prognostic impact of stroke. Of 4 240 284 HDP delivery hospitalizations, 3391 (0.08%) women had stroke. While the prevalence of HDP increased over time, incident stroke rates decreased from 10 to 6 per 10 000 HDP delivery hospitalizations between 2004 and 2014. Women with stroke were increasingly multimorbid, with some risk factors being more strongly associated with ischemic strokes, including congenital heart disease, peripheral vascular disease, dyslipidemia, and sickle cell disease. Delivery complications were also associated with stroke, including cesarean section (odds ratio [OR], 1.58; 95% CI, 1.33-1.86), postpartum hemorrhage (OR, 1.91; 95% CI, 1.33-1.86), and maternal mortality (OR, 99.78; 95% CI, 59.15-168.31), independently of potential confounders. Women with stroke had longer hospital stays (median, 6 versus 3 days), higher hospital charges (median, $14 655 versus $4762), and a higher proportion of nonroutine discharge locations (38% versus 4%). Conclusions The incidence of stroke in women with HDP has declined over time. While a relatively rare event, identification of women at highest risk of ischemic or hemorrhagic stroke on admission for delivery is important to reduce long-term sequelae.
Keywords: preeclampsia/pregnancy; pregnancy; stroke in young adults.
Conflict of interest statement
None.
Figures

Comment in
-
Are Strokes Declining Among Pregnant Women With Hypertensive Disorders of Pregnancy?J Am Heart Assoc. 2020 Aug 4;9(15):e017917. doi: 10.1161/JAHA.120.017917. Epub 2020 Jul 29. J Am Heart Assoc. 2020. PMID: 32750293 Free PMC article. No abstract available.
References
-
- McClure JH, Cooper GM, Clutton‐Brock TH. Saving mothers’ lives: reviewing maternal deaths to make motherhood safer: 2006–8: a review. Br J Anaesth. 2011;107:127–132. - PubMed
-
- Say L, Chou D, Gemmill A, Tuncalp O, Moller AB, Daniels J, Gulmezoglu AM, Temmerman M, Alkema L. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323–e333. - PubMed
-
- Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102:181–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
