

Determinants of Pericoronary Adipose Tissue Attenuation on Computed Tomography Angiography in Coronary Artery Disease
- PMID: 32750306
- PMCID: PMC7792233
- DOI: 10.1161/JAHA.120.016202
Determinants of Pericoronary Adipose Tissue Attenuation on Computed Tomography Angiography in Coronary Artery Disease
Abstract
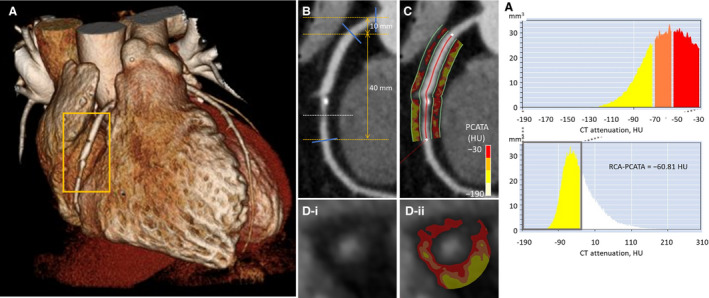
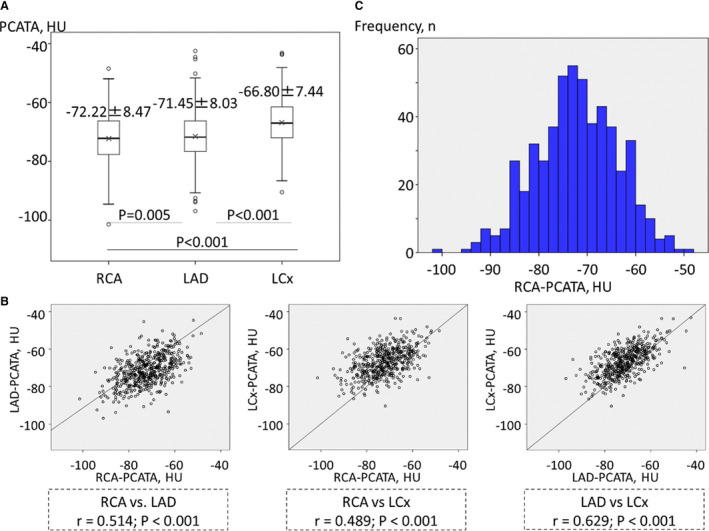
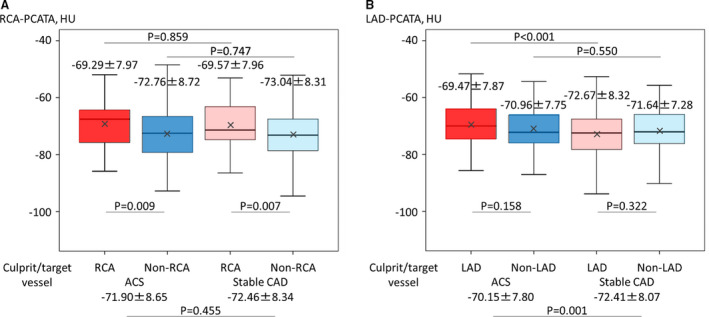
Background Recent studies have reported the association between pericoronary inflammation assessed by pericoronary adipose tissue attenuation (PCATA) on computed tomography angiography and worse outcomes in patients with coronary artery disease. We investigated the determinants predicting increased PCATA in patients with known or suspected coronary artery disease. Methods and Results A total of 540 patients who underwent computed tomography angiography and invasive coronary angiography were studied. Mean computed tomography attenuation values of PCAT (-190 to -30 Hounsfield units) (PCATA) were assessed at the proximal 40-mm segments of all 3 major coronary arteries by crude analysis. Univariable and multivariable analyses were performed to determine the predictors of increased PCATA surrounding the proximal right coronary artery. Mean right coronary artery-PCATA was -72.22±8.47 Hounsfield units and the average of 3-vessel PCATA was -70.24±6.60 Hounsfield units. Multivariable linear regression analysis revealed that the independent determinants of right coronary artery-PCATA were male (β coefficient=4.965, P<0.001), left ventricular mass index (β coefficient=0.040, P=0.025), and angiographically significant stenosis (diameter stenosis >50%) (β coefficient=2.418, P=0.008). Sex-related determinants were NT-proBNP level (N-terminal pro-B-type natriuretic peptide; β coefficient <0.001, P=0.026), Agatston score (β coefficient=-0.002, P=0.010), left ventricular mass index (β coefficient=0.041, P=0.028), and significant stenosis (β coefficient=4.006, P<0.001) in male patients and left ventricular ejection fraction (β coefficient=-0.217, P=0.010) and significant stenosis (β coefficient=3.835, P=0.023) in female patients. Conclusions Right coronary artery-PCATA was associated with multiple clinical characteristics, established risk factors, and the presence of significant stenosis. Our results suggest that clinically significant factors such as sex, left ventricular hypertrophy, ejection fraction, calcification, and epicardial stenosis should be taken into account in the assessment of pericoronary inflammation using computed tomography angiography.
Keywords: adipose tissue; computed tomography angiography; coronary artery disease; inflammation.
Conflict of interest statement
None.
Figures
Similar articles
-
Impact of pericoronary adipose tissue inflammation on left ventricular hypertrophy and regional physiological indices in stable coronary artery disease patients with preserved systolic function.Heart Vessels. 2021 Jan;36(1):24-37. doi: 10.1007/s00380-020-01658-1. Epub 2020 Jul 8. Heart Vessels. 2021. PMID: 32638076
-
Pericoronary adipose tissue attenuation predicts compositional plaque changes: a 12-month longitudinal study in individuals with type 2 diabetes without symptoms or known coronary artery disease.Cardiovasc Diabetol. 2025 Mar 28;24(1):143. doi: 10.1186/s12933-025-02694-9. Cardiovasc Diabetol. 2025. PMID: 40155929 Free PMC article.
-
Association of perivascular fat attenuation on computed tomography and heart failure with preserved ejection fraction.ESC Heart Fail. 2023 Aug;10(4):2447-2457. doi: 10.1002/ehf2.14419. Epub 2023 May 31. ESC Heart Fail. 2023. PMID: 37259241 Free PMC article.
-
The Emerging Role of CT-Based Imaging in Adipose Tissue and Coronary Inflammation.Cells. 2021 May 13;10(5):1196. doi: 10.3390/cells10051196. Cells. 2021. PMID: 34068406 Free PMC article. Review.
-
Evaluation of pericoronary adipose tissue attenuation on CT.Br J Radiol. 2023 Apr 1;96(1145):20220885. doi: 10.1259/bjr.20220885. Epub 2023 Jan 23. Br J Radiol. 2023. PMID: 36607825 Free PMC article. Review.
Cited by
-
Coronary Computed Tomography Angiographic Predictors of Non-culprit Territory Unrecognized Myocardial Infarction Assessed by Cardiac Magnetic Resonance in Non-ST-elevation Acute Coronary Syndrome.Front Cardiovasc Med. 2022 Jan 31;8:825523. doi: 10.3389/fcvm.2021.825523. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35174226 Free PMC article.
-
Relationship of OCT-defined plaque characteristics with CCTA-derived coronary inflammation and CMR-derived global coronary flow reserve in patients with acute coronary syndrome.PLoS One. 2023 May 25;18(5):e0286196. doi: 10.1371/journal.pone.0286196. eCollection 2023. PLoS One. 2023. PMID: 37228044 Free PMC article.
-
Evaluation of Pericoronary Fat Attenuation Index to Better Identify Culprit Lesions in Acute Coronary Syndrome According to Stenosis Severity.J Comput Assist Tomogr. 2025 Jan-Feb 01;49(1):93-100. doi: 10.1097/RCT.0000000000001661. Epub 2024 Sep 11. J Comput Assist Tomogr. 2025. PMID: 39284101 Free PMC article.
-
A systematic review exploring the significance of measuring epicardial fat thickness in correlation to B-type natriuretic peptide levels as prognostic and diagnostic markers in patients with or at risk of heart failure.Heart Fail Rev. 2022 Mar;27(2):665-675. doi: 10.1007/s10741-021-10160-3. Epub 2021 Oct 20. Heart Fail Rev. 2022. PMID: 34671870 Free PMC article.
-
Estimating inflammatory risk in atherosclerotic cardiovascular disease: plaque over plasma?Eur Heart J Cardiovasc Imaging. 2025 Mar 3;26(3):444-460. doi: 10.1093/ehjci/jeae314. Eur Heart J Cardiovasc Imaging. 2025. PMID: 39657321 Free PMC article. Review.
References
-
- Ross R. Atherosclerosis–an inflammatory disease. N Engl J Med. 1999;340:115–126. - PubMed
-
- Mazurek T, Zhang L, Zalewski A, Mannion JD, Diehl JT, Arafat H, Sarov‐Blat L, O'Brien S, Keiper EA, Johnson AG, et al. Human epicardial adipose tissue is a source of inflammatory mediators. Circulation. 2003;108:2460–2466. - PubMed
-
- Shimabukuro M, Hirata Y, Tabata M, Dagvasumberel M, Sato H, Kurobe H, Fukuda D, Soeki T, Kitagawa T, Takanashi S, et al. Epicardial adipose tissue volume and adipocytokine imbalance are strongly linked to human coronary atherosclerosis. Arterioscler Thromb Vasc Biol. 2013;33:1077–1084. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
