

Associations of Left Ventricular Structure and Function With Blood Pressure in Heart Failure With Preserved Ejection Fraction: Analysis of the TOPCAT Trial
- PMID: 32750310
- PMCID: PMC7792255
- DOI: 10.1161/JAHA.119.016009
Associations of Left Ventricular Structure and Function With Blood Pressure in Heart Failure With Preserved Ejection Fraction: Analysis of the TOPCAT Trial
Abstract
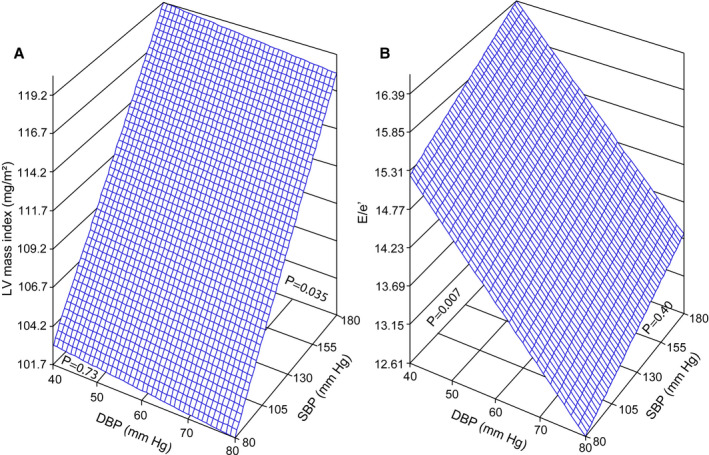
Background Data on the association of systolic and diastolic blood pressure with the structure and function of failing hearts with preserved ejection fraction (EF) are sparse. Methods and Results This analysis included 935 patients with heart failure (49.4% women; mean age, 69.9 years) with preserved EF (≥45%) enrolled in the TOPCAT (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist) Trial before initiation of randomized therapy. Left ventricular (LV) structure (dimensions, wall thickness, and mass index), diastolic function (left atrial volume index, transmitral blood flow, and mitral annular velocities), and systolic function (EF and longitudinal strain) were assessed echocardiographically. In multivariable-adjusted analyses, association sizes expressed per 1-SD (14.8-mm Hg) increment in systolic blood pressure were 0.020 cm (P=0.003) and 0.018 cm (P=0.004) for LV septal and posterior wall thickness, respectively, and 2.42 mg/m2 (P=0.018) for LV mass index. The corresponding associations with diastolic blood pressure were nonsignificant (P≥0.067). In similarly adjusted analyses, the association sizes expressed per 1-SD (10.7-mm Hg) increment in diastolic blood pressure were -0.15 for E/A (P<0.001), -0.76 for E/e' (P=0.006), and -0.62% for EF (P=0.024). These findings were consistent, if models including systolic blood pressure were additionally adjusted for diastolic blood pressure and vice versa, albeit that the relation of EF with diastolic blood pressure weakened (-0.54%; P=0.10). Conclusions In diastolic heart failure, LV wall thickness and LV mass index increased with higher systolic blood pressure, but not with higher diastolic blood pressure, whereas functional measures reflecting diastolic LV function decreased with higher diastolic blood pressure, independent of systolic blood pressure. These observations highlight the importance of controlling both systolic and diastolic blood pressure as modifiable risk factors to reduce the risk of LV remodeling and diastolic LV dysfunction.
Keywords: blood pressure; diastolic heart failure; echocardiography; hypertension; left ventricle.
Figures
References
-
- Li Y, Staessen JA, Sheng CS, Huang QF, O'Rourke M, Wang JG. Age dependency of peripheral and central systolic pressures: cross‐sectional and longitudinal observations in a Chinese population. Hypertens Res. 2012;115–122. - PubMed
-
- Clement DL, De Buyzere ML, De Bacquer DA, de Leeuw PW, Duprez DA, Fagard RH, Gheeraert PJ, Missault LH, Braun JJ, Six RO, et al. Prognostic value of ambulatory blood‐pressure recordings in patients with treated hypertension. N Engl J Med. 2003;2407–2415. - PubMed
-
- Sheppard JP, Tucker KL, Davison WJ, Stevens R, Aekplakorn W, Bosworth HB, Bove A, Earle K, Godwin M, Green BB, et al. Self‐monitoring of blood pressure in patients with hypertension‐related multi‐morbidity: systematic review and individual patient data meta‐analysis. Am J Hypertens. 2019;243–251. - PMC - PubMed
-
- Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, Chalmers J, Rodgers A, Rahimi K. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta‐analysis. Lancet. 2016;957–967. - PubMed
-
- Kannel WB, Schwartz MJ, McNamara PM. Blood pressure and risk of cardiovascular disease: the Framingham Heart Study. Chest. 1969;43–51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
