

Noninvasive Prediction of Elevated Wedge Pressure in Pulmonary Hypertension Patients Without Clear Signs of Left-Sided Heart Disease: External Validation of the OPTICS Risk Score
- PMID: 32750312
- PMCID: PMC7792270
- DOI: 10.1161/JAHA.119.015992
Noninvasive Prediction of Elevated Wedge Pressure in Pulmonary Hypertension Patients Without Clear Signs of Left-Sided Heart Disease: External Validation of the OPTICS Risk Score
Abstract
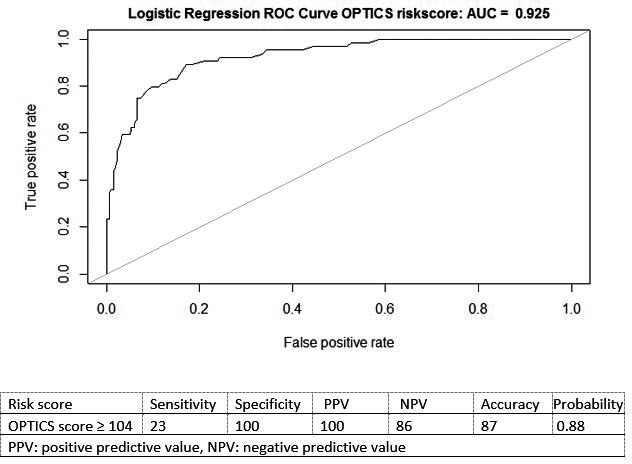
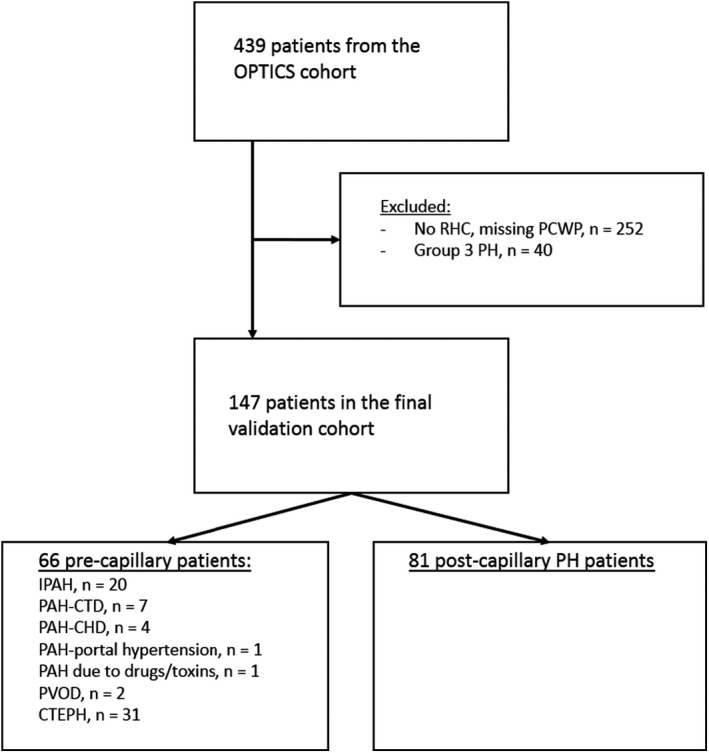
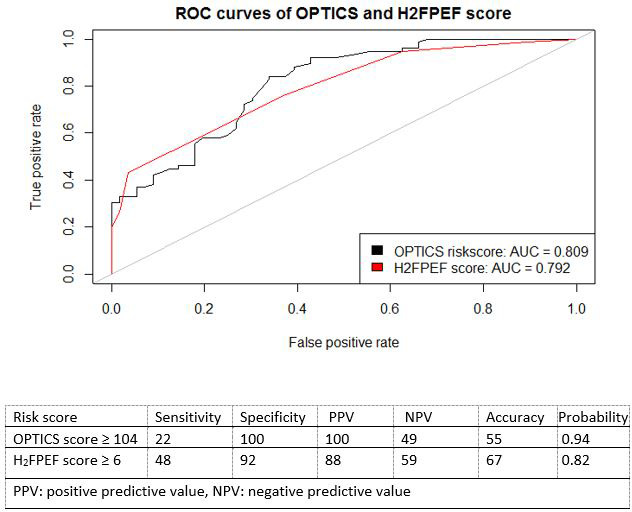
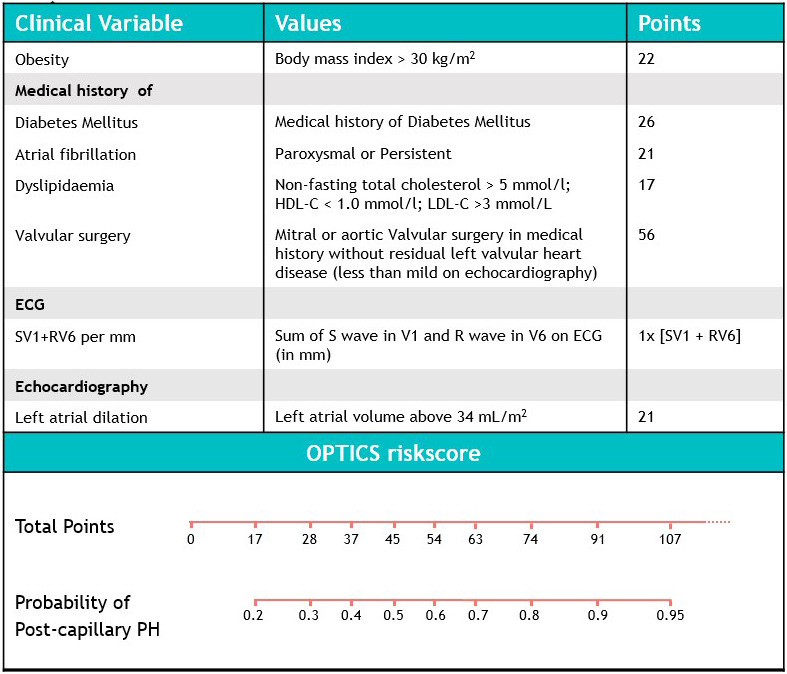
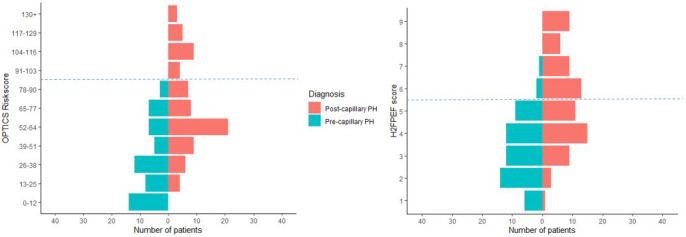
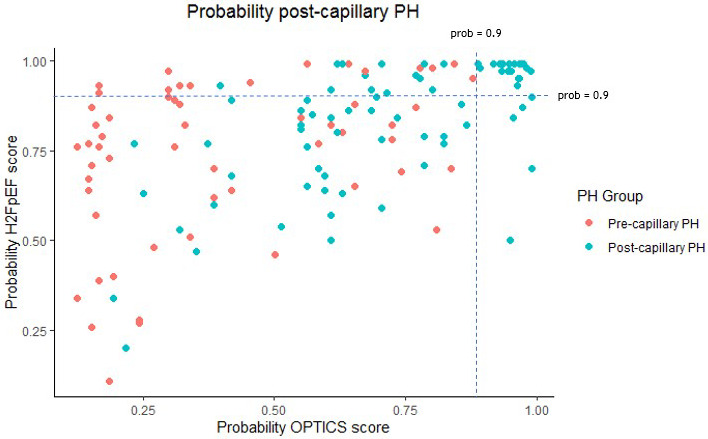
Background Although most newly presenting patients with pulmonary hypertension (PH) have elevated pulmonary artery wedge pressure, identification of so-called postcapillary PH can be challenging. A noninvasive tool predicting elevated pulmonary artery wedge pressure in patients with incident PH may help avoid unnecessary invasive diagnostic procedures. Methods and Results A combination of clinical data, ECG, and echocardiographic parameters was used to refine a previously developed left heart failure risk score in a retrospective cohort of pre- and postcapillary PH patients. This updated score (renamed the OPTICS risk score) was externally validated in a prospective cohort of patients from 12 Dutch nonreferral centers the OPTICS network. Using the updated OPTICS risk score, the presence of postcapillary PH could be predicted on the basis of body mass index ≥30, diabetes mellitus, atrial fibrillation, dyslipidemia, history of valvular surgery, sum of SV1 (deflection in V1 in millimeters) and RV6 (deflection in V6 in millimeters) on ECG, and left atrial dilation. The external validation cohort included 81 postcapillary PH patients and 66 precapillary PH patients. Using a predefined cutoff of >104, the OPTICS score had 100% specificity for postcapillary PH (sensitivity, 22%). In addition, we investigated whether a high probability of heart failure with preserved ejection fraction, assessed by the H2FPEF score (obesity, atrial fibrillation, age >60 yrs, ≥2 antihypertensives, E/e' >9, and pulmonary artery systolic pressure by echo >35 mmHg), similarly predicted the presence of elevated pulmonary artery wedge pressure. High probability of heart failure with preserved ejection fraction (H2FPEF score ≥6) was less specific for postcapillary PH. Conclusions In a community setting, the OPTICS risk score can predict elevated pulmonary artery wedge pressure in PH patients without clear signs of left-sided heart disease. The OPTICS risk score may be used to tailor the decision to perform invasive diagnostic testing.
Keywords: diagnosis; heart failure; prediction models; pulmonary vasculature; validation study.
Figures
Comment in
-
Clearing Our Vision for Discerning Precapillary From Postcapillary Pulmonary Hypertension With the OPTICS Risk Score.J Am Heart Assoc. 2020 Aug 4;9(15):e017685. doi: 10.1161/JAHA.120.017685. Epub 2020 Jul 31. J Am Heart Assoc. 2020. PMID: 32750289 Free PMC article. No abstract available.
References
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;343–349. - PubMed
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015;903–975. - PubMed
-
- Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite‐Moreira AF, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;2539–2550. - PubMed
-
- Gall H, Felix JF, Schneck FK, Milger K, Sommer N, Voswinckel R, Franco OH, Hofman A, Schermuly RT, Weissmann N, et al. The Giessen Pulmonary Hypertension Registry: survival in pulmonary hypertension subgroups. J Heart Lung Transplant. 2017;957–967. - PubMed
-
- Deano RC, Glassner‐Kolmin C, Rubenfire M, Frost A, Visovatti S, McLaughlin VV, Gomberg‐Maitland M. Referral of patients with pulmonary hypertension diagnoses to tertiary pulmonary hypertension centers: the multicenter RePHerral study. JAMA Intern Med. 2013;887–893. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
