

Medium-Term Complications Associated With Coronary Artery Aneurysms After Kawasaki Disease: A Study From the International Kawasaki Disease Registry
- PMID: 32750313
- PMCID: PMC7792232
- DOI: 10.1161/JAHA.119.016440
Medium-Term Complications Associated With Coronary Artery Aneurysms After Kawasaki Disease: A Study From the International Kawasaki Disease Registry
Abstract
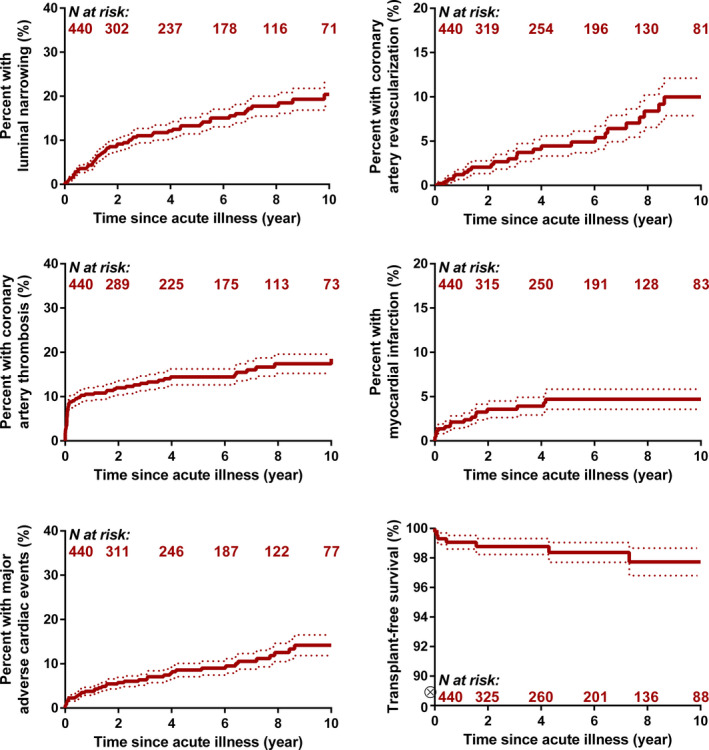
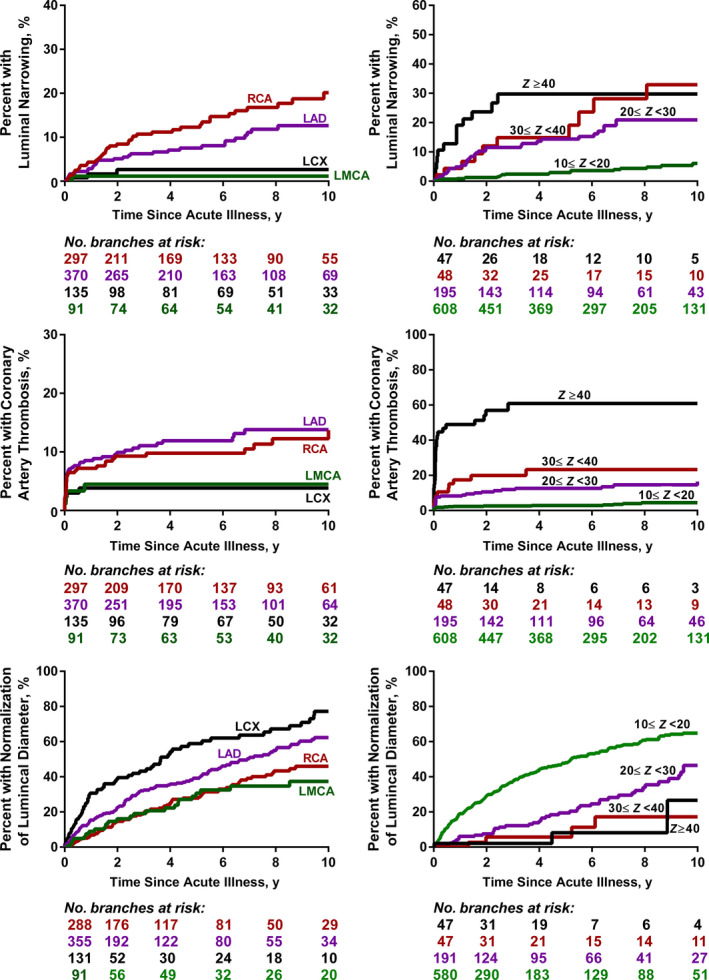
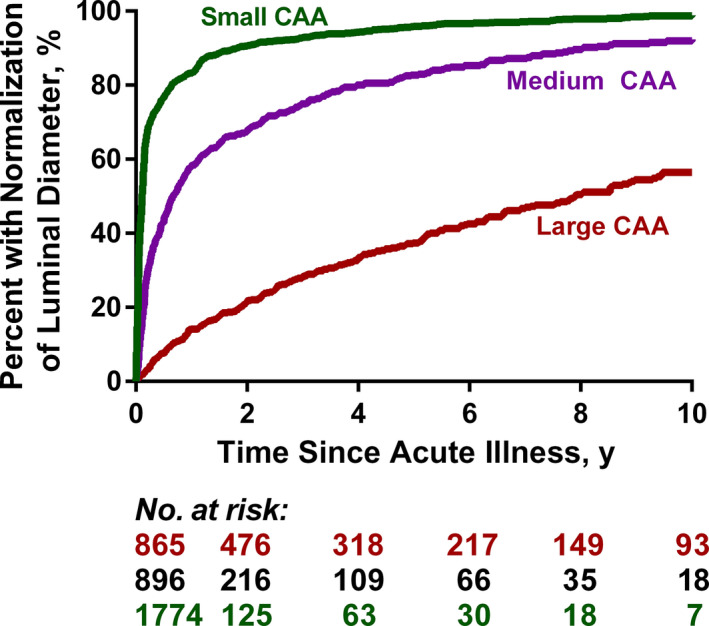
Background Coronary artery aneurysms (CAAs) may occur after Kawasaki disease (KD) and lead to important morbidity and mortality. As CAA in patients with KD are rare and heterogeneous lesions, prognostication and risk stratification are difficult. We sought to derive the cumulative risk and associated factors for cardiovascular complications in patients with CAAs after KD. Methods and Results A 34-institution international registry of 1651 patients with KD who had CAAs (maximum CAA Z score ≥2.5) was used. Time-to-event analyses were performed using the Kaplan-Meier method and Cox proportional hazard models for risk factor analysis. In patients with CAA Z scores ≥10, the cumulative incidence of luminal narrowing (>50% of lumen diameter), coronary artery thrombosis, and composite major adverse cardiovascular complications at 10 years was 20±3%, 18±2%, and 14±2%, respectively. No complications were observed in patients with a CAA Z score <10. Higher CAA Z score and a greater number of coronary artery branches affected were associated with increased risk of all types of complications. At 10 years, normalization of luminal diameter was noted in 99±4% of patients with small (2.5≤Z<5.0), 92±1% with medium (5.0≤Z<10), and 57±3% with large CAAs (Z≥10). CAAs in the left anterior descending and circumflex coronary artery branches were more likely to normalize. Risk factor analysis of coronary artery branch level outcomes was performed with a total of 893 affected branches with Z score ≥10 in 440 patients. In multivariable regression models, hazards of luminal narrowing and thrombosis were higher for patients with CAAs of the right coronary artery and left anterior descending branches, those with CAAs that had complex architecture (other than isolated aneurysms), and those with CAAs with Z scores ≥20. Conclusions For patients with CAA after KD, medium-term risk of complications is confined to those with maximum CAA Z scores ≥10. Further risk stratification and close follow-up, including advanced imaging, in patients with large CAAs is warranted.
Keywords: Kawasaki disease; cardiovascular outcomes; coronary artery; risk factors.
Conflict of interest statement
None.
Figures
References
-
- McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, Baker AL, Jackson MA, Takahashi M, Shah PB, et al. Diagnosis, treatment, an d long‐term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135:e927–e999. - PubMed
-
- McCrindle BW, Li JS, Minich LL, Colan SD, Atz AM, Takahashi M, Vetter VL, Gersony WM, Mitchell PD, Newburger JW, et al.; Pediatric Heart Network Investigators . Coronary artery involvement in children with Kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation. 2007;116:174–179. - PubMed
-
- Suzuki A, Kamiya T, Kuwahara N, Ono Y, Kohata T, Takahashi O, Kimura K, Takamiya M. Coronary arterial lesions of Kawasaki disease: cardiac catheterization findings of 1100 cases. Pediatr Cardiol. 1986;7:3–9. - PubMed
-
- Kato H, Sugimura T, Akagi T, Sato N, Hashino K, Maeno Y, Kazue T, Eto G, Yamakawa R. Long‐term consequences of Kawasaki disease. A 10‐ to 21‐year follow‐up study of 594 patients. Circulation. 1996;94:1379–1385. - PubMed
