

Can Health Disparity Be Eliminated? The Role of Family Doctor Played in Shanghai, China
- PMID: 32751946
- PMCID: PMC7432843
- DOI: 10.3390/ijerph17155548
Can Health Disparity Be Eliminated? The Role of Family Doctor Played in Shanghai, China
Abstract
Background: Globally, the elimination of health disparity is a significant policy target. Primary health care has been implemented as a strategy to achieve this target in China for almost 10 years. This study examined whether family doctor (FD) policy in Shanghai contributed to eliminating health disparity as expected.
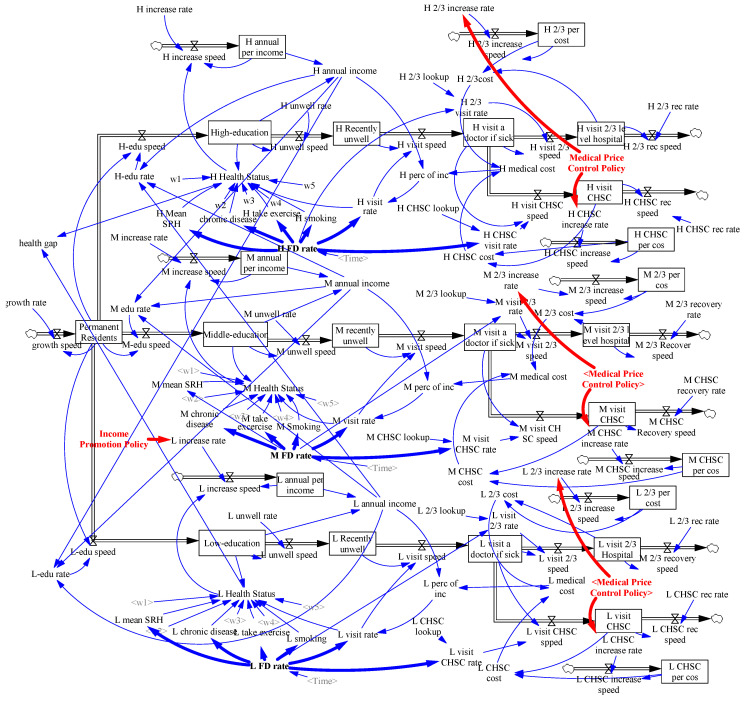
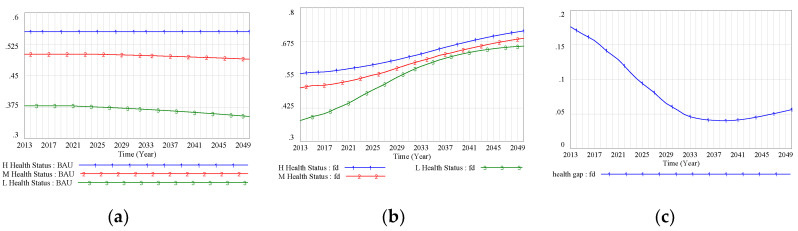
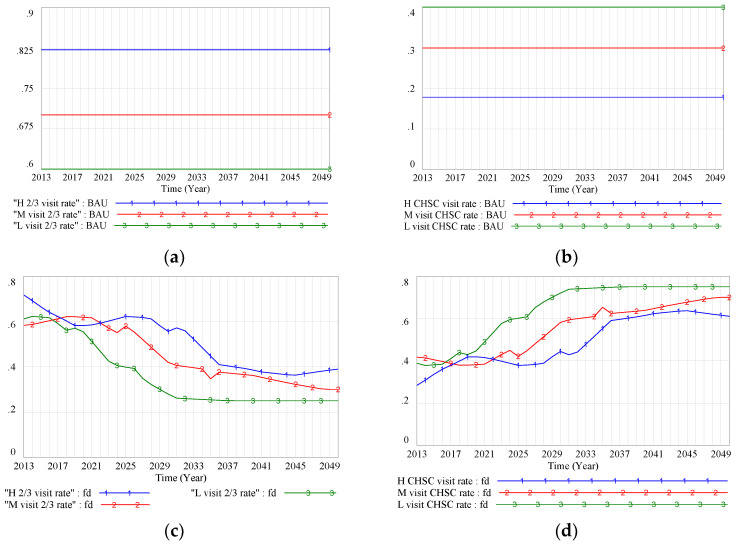
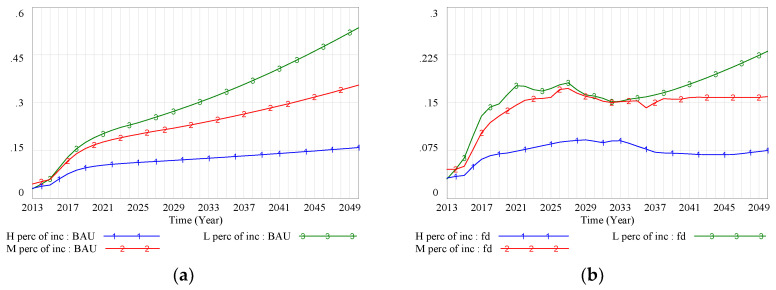
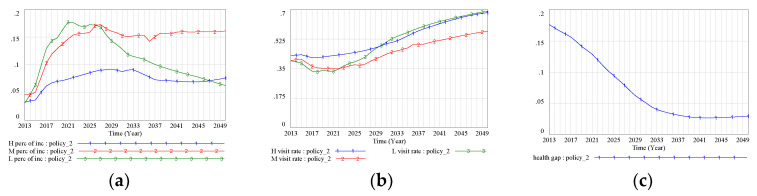
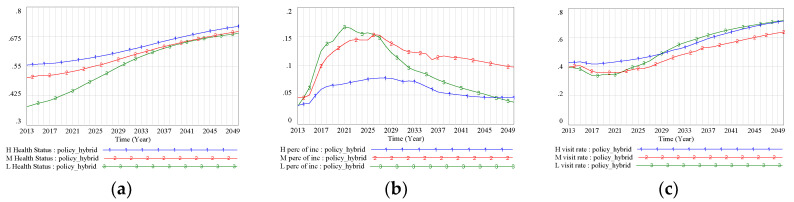
Methods: System dynamics modeling was performed to construct and simulate a system of health disparity formation (business-as-usual (BAU) scenario, without any interventions), a system with FD intervention (FD scenario), and three other systems with supporting policies (Policy 1/Policy 2/Policy hybrid scenario) from 2013 to 2050. Health disparities were simulated in different scenarios, making it possible to compare the BAU results with those of FD intervention and with other policy interventions.
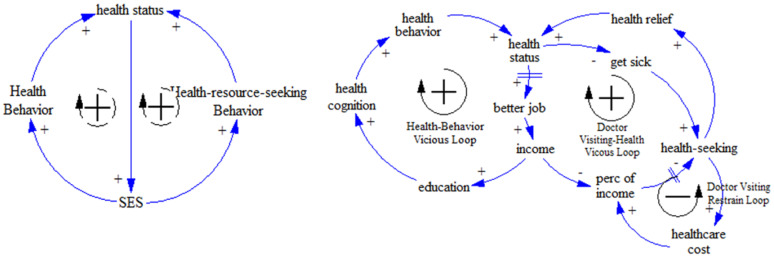
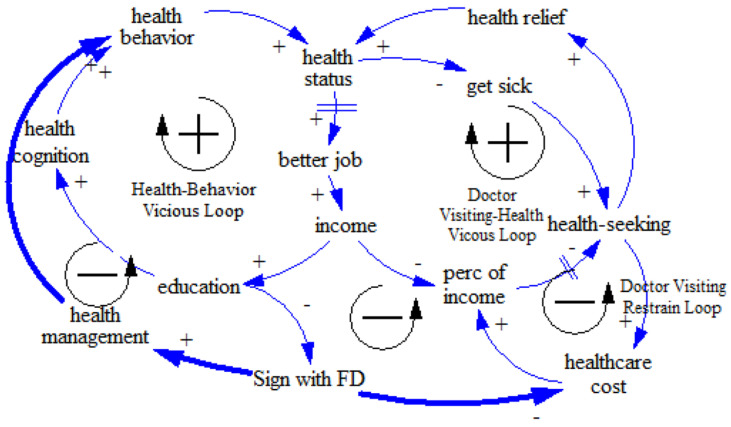
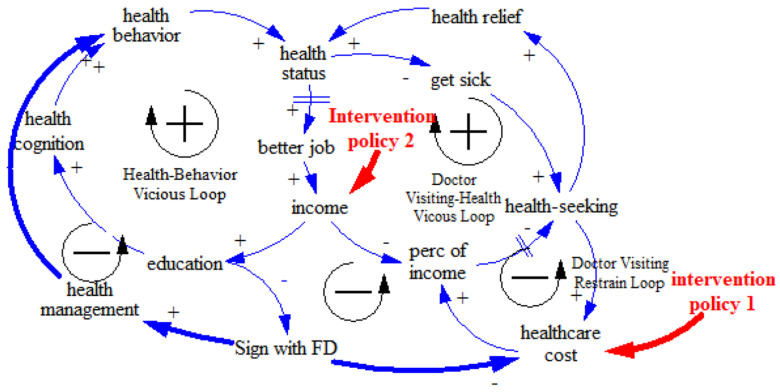
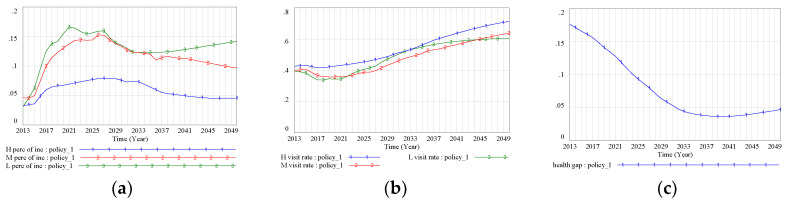
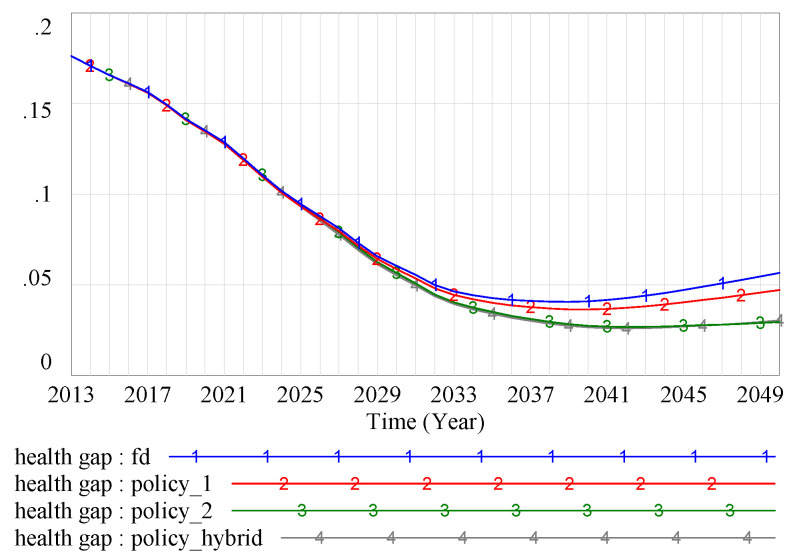
Findings: System dynamics models showed that the FD policy would play a positive role in reducing health disparities in the initial stage, and medical price control-rather than health management-was the dominant mechanism. However, in this model, the health gap was projected to expand again around 2039. The model examined the introduction of two intervention policies, with findings showing that the policy focused on socioeconomic status improvement would be more effective in reducing health disparities, suggesting that socioeconomic status is the fundamental cause of these disparities.
Conclusions: The results indicate that health disparities could be optimized, but not eliminated, as long as differences in socioeconomic status persists.
Keywords: China; family doctor; health disparity; socioeconomic status; system dynamics modeling.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The effect of family doctor policy practice on primary health-care workers' health in Hongkou District of Shanghai, China: varied by occupational divisions?BMC Fam Pract. 2020 Sep 30;21(1):205. doi: 10.1186/s12875-020-01275-x. BMC Fam Pract. 2020. PMID: 32998704 Free PMC article.
-
Can family doctor contracted services facilitate orderly visits in the referral system? A frontier policy study from Shanghai, China.Int J Health Plann Manage. 2022 Jan;37(1):403-416. doi: 10.1002/hpm.3346. Epub 2021 Oct 9. Int J Health Plann Manage. 2022. PMID: 34628680 Free PMC article.
-
Multilevel Examination of Health Disparity: The Role of Policy Implementation in Neighborhood Context, in Patient Resources, and in Healthcare Facilities on Later Stage of Breast Cancer Diagnosis.Cancer Epidemiol Biomarkers Prev. 2019 Jan;28(1):59-66. doi: 10.1158/1055-9965.EPI-17-0945. Epub 2018 Oct 23. Cancer Epidemiol Biomarkers Prev. 2019. PMID: 30352817 Free PMC article.
-
Health disparities in chronic kidney disease: are we making any progress?Nephrol News Issues. 2009 Apr;23(4):48, 50-1. Nephrol News Issues. 2009. PMID: 19437948 Review.
-
Achieving Health Equity: Closing The Gaps In Health Care Disparities, Interventions, And Research.Health Aff (Millwood). 2016 Aug 1;35(8):1410-5. doi: 10.1377/hlthaff.2016.0158. Health Aff (Millwood). 2016. PMID: 27503965 Review.
Cited by
-
Effects of Healthcare Policies and Reforms at the Primary Level in China: From the Evidence of Shenzhen Primary Care Reforms from 2018 to 2019.Int J Environ Res Public Health. 2022 Feb 9;19(4):1945. doi: 10.3390/ijerph19041945. Int J Environ Res Public Health. 2022. PMID: 35206133 Free PMC article.
-
Impact of family doctor contracted services on the health of migrants: a cross-sectional study in China.Sci Rep. 2024 Nov 27;14(1):29510. doi: 10.1038/s41598-024-81068-9. Sci Rep. 2024. PMID: 39604578 Free PMC article.
-
Does a GP service package matter in addressing the absence of health management by the occupational population? A modelling study.BMC Health Serv Res. 2024 May 17;24(1):638. doi: 10.1186/s12913-024-10954-9. BMC Health Serv Res. 2024. PMID: 38760746 Free PMC article.
-
A spatial feature analysis of primary health care utilization in a large city in China and its implications for family doctor contract service policy.BMC Health Serv Res. 2024 Feb 13;24(1):194. doi: 10.1186/s12913-023-10389-8. BMC Health Serv Res. 2024. PMID: 38351077 Free PMC article.
-
Can family doctor system improve health service utilization for patients with hypertension and diabetes in China? A difference-in-differences study.BMC Health Serv Res. 2024 Apr 11;24(1):454. doi: 10.1186/s12913-024-10903-6. BMC Health Serv Res. 2024. PMID: 38605337 Free PMC article.
References
-
- Department of Health and Social Security . Inequalities in Health: Report of A Research Working Group. DHSS; London, UK: 1980.
-
- Wagstaff A., Van Doorslaer E., Watanabe N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J. Econom. 2003;112:207–223. doi: 10.1016/S0304-4076(02)00161-6. - DOI
-
- Robert S.A., House J.S. Socioeconomic inequalities in health: An enduring sociological problem. Handb. Med. Sociol. 2000;5:79–97.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
