

Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform
- PMID: 32751954
- PMCID: PMC7464346
- DOI: 10.3390/brainsci10080504
Distinguishing and Biochemical Phenotype Analysis of Epilepsy Patients Using a Novel Serum Profiling Platform
Abstract
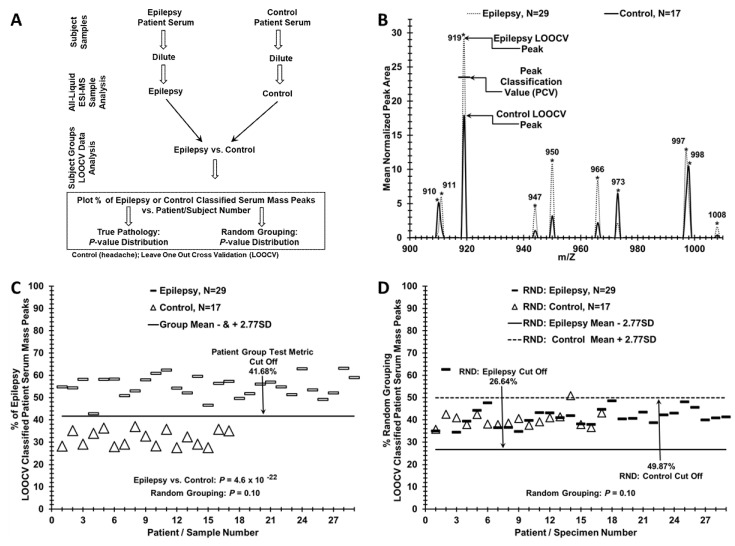
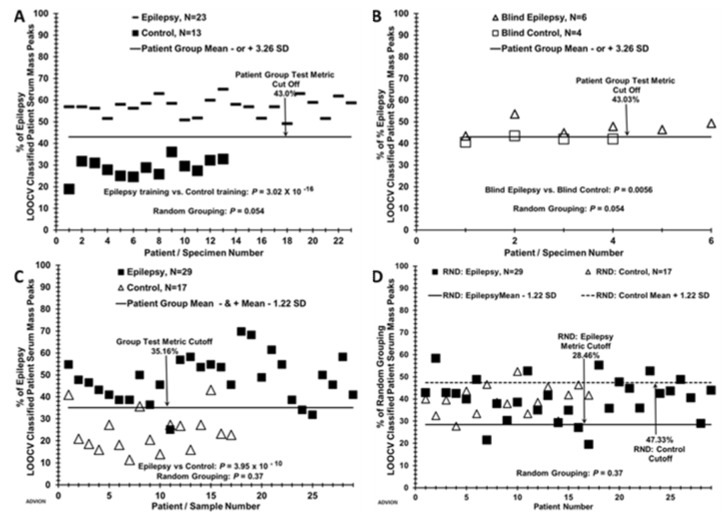
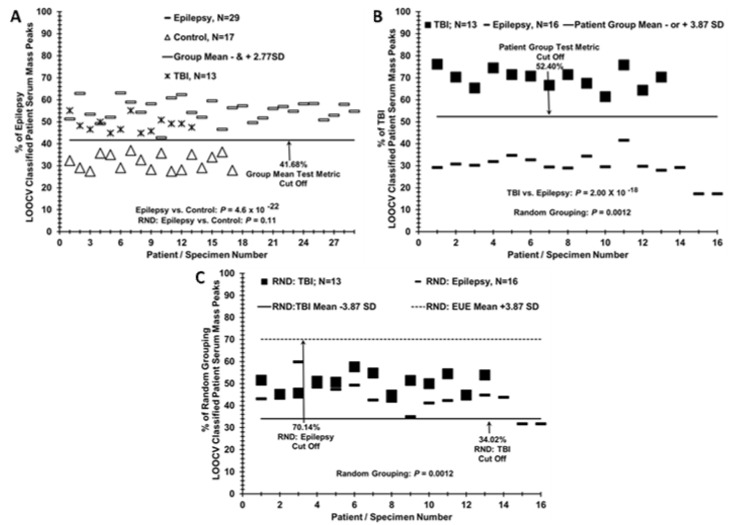
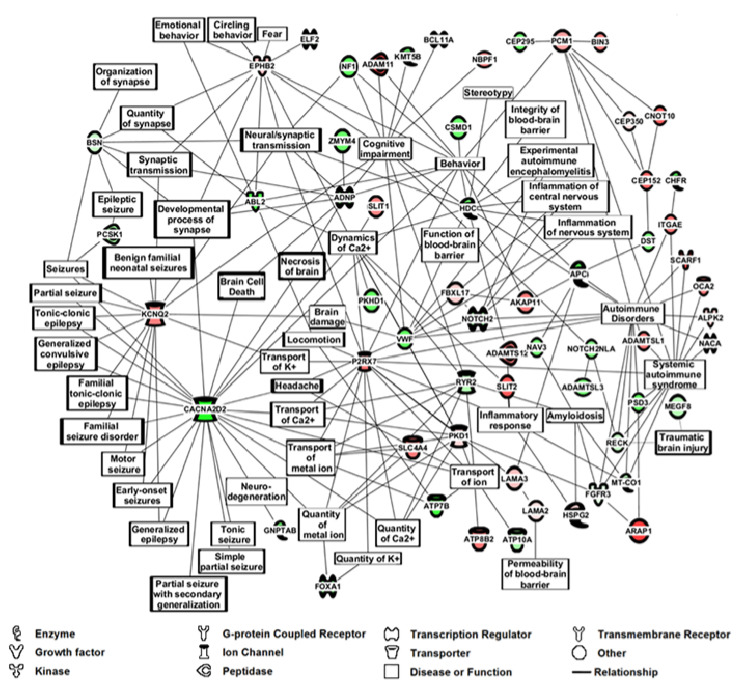
Diagnosis of non-symptomatic epilepsy includes a history of two or more seizures and brain imaging to rule out structural changes like trauma, tumor, infection. Such analysis can be problematic. It is important to develop capabilities to help identify non-symptomatic epilepsy in order to better monitor and understand the condition. This understanding could lead to improved diagnostics and therapeutics. Serum mass peak profiling was performed using electrospray ionization mass spectrometry (ESI-MS). A comparison of sera mass peaks between epilepsy and control groups was performed via leave one [serum sample] out cross-validation (LOOCV). MS/MS peptide analysis was performed on serum mass peaks to compare epilepsy patient and control groups. LOOCV identified significant differences between the epilepsy patient group and control group (p = 10-22). This value became non-significant (p = 0.10) when the samples were randomly allocated between the groups and reanalyzed by LOOCV. LOOCV was thus able to distinguish a non-symptomatic epilepsy patient group from a control group based on physiological differences and underlying phenotype. MS/MS was able to identify potential peptide/protein changes involved in this epilepsy versus control comparison, with 70% of the top 100 proteins indicating overall neurologic function. Specifically, peptide/protein sera changes suggested neuro-inflammatory, seizure, ion-channel, synapse, and autoimmune pathways changing between epilepsy patients and controls.
Keywords: epilepsy; mass spectrometry; monitoring; phenotype analysis; serum profiling.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
Grants and funding
- R21NS077466/National Institute of Neurological Diseases and Stroke in the U.S.
- BT/MB/BRCP/06/2011/The Department of Biotechnology in India under the U.S.-India Bilateral Brain Research Collaborative Partnerships (U.S. - India BRCP).
- R01NS098891/The National Institute of Neurological Diseases and Stroke and the Fogarty International Center under the Global Brain and Nervous System Disorders Research Across the Lifespan program.
- 829-VREF/Veterans Administration Research and Education Fund
- W81XWH-16-1-0295/U.S. Department of Defense
LinkOut - more resources
Full Text Sources
