

GlycA Levels during the Earliest Stages of Rheumatoid Arthritis: Potential Use as a Biomarker of Subclinical Cardiovascular Disease
- PMID: 32752190
- PMCID: PMC7463667
- DOI: 10.3390/jcm9082472
GlycA Levels during the Earliest Stages of Rheumatoid Arthritis: Potential Use as a Biomarker of Subclinical Cardiovascular Disease
Abstract
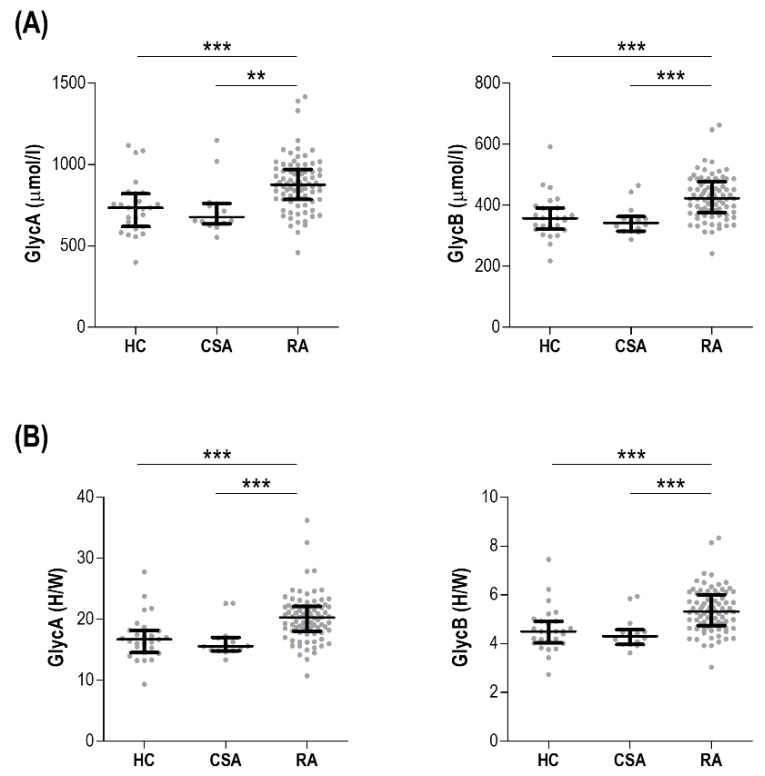
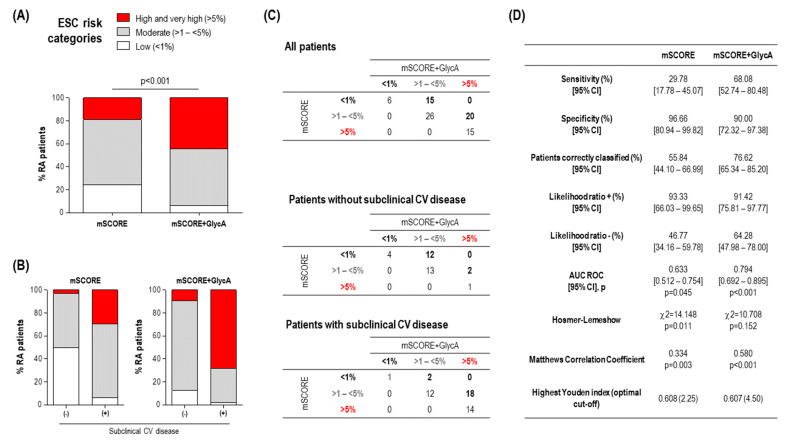
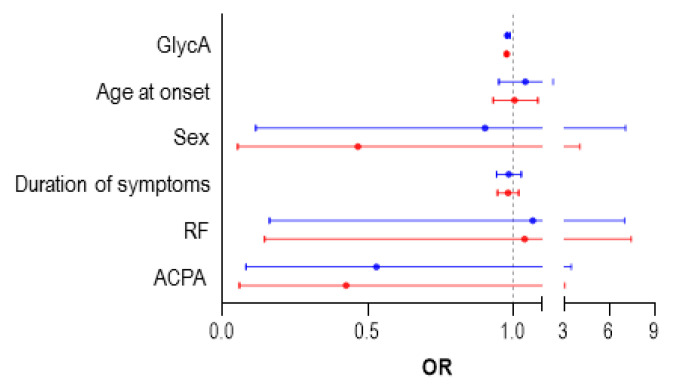
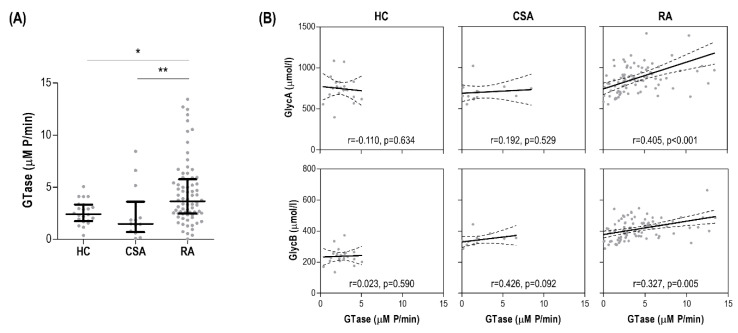
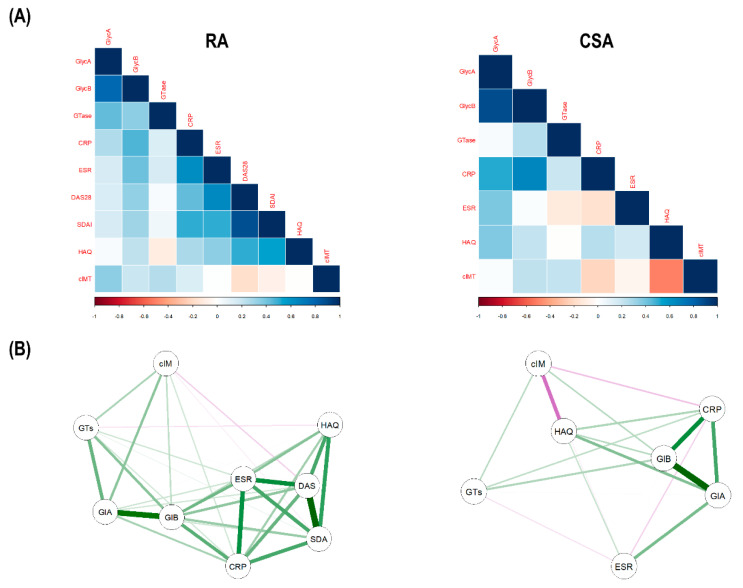
This study aimed at evaluating the clinical relevance of glycoprotein profiles during the earliest phases of rheumatoid arthritis (RA) as biomarkers of cardiovascular (CV) risk and treatment response. Then, GlycA and GlycB serum levels were measured using 1H-nuclear magnetic resonance in 82 early RA patients, 14 clinically-suspect arthralgia (CSA), and 28 controls. Serum glycosyltransferase activity was assessed by a colorimetric assay. Subclinical CV disease was assessed by Doppler-ultrasound. We found that GlycA and GlycB serum levels were increased in RA (both p < 0.001), but not in CSA, independently of cardiometabolic risk factors. Increased serum glycosyltransferase activity paralleled GlycA (r = 0.405, p < 0.001) and GlycB levels (r = 0.327, p = 0.005) in RA. GlycA, but not GlycB, was associated with atherosclerosis occurrence (p = 0.012) and severity (p = 0.001). Adding GlycA to the mSCORE improved the identification of patients with atherosclerosis over mSCORE alone, increasing sensitivity (29.7 vs. 68.0%) and accuracy (55.8 vs. 76.6%) and allowing reclassification into more appropriate risk categories. GlycA-reclassification identified patients with impaired lipoprotein metabolism. Finally, baseline GlycA levels predicted poor clinical response upon anti-rheumatic treatment at 6 and 12 months in univariate and multivariate analysis. In sum, increased GlycA levels during the earliest stage of RA can be considered a powerful biomarker for CV risk stratification and treatment response.
Keywords: H-NMR; atherosclerosis; cardiovascular risk; early rheumatoid arthritis; glycoproteins; inflammation.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Amigó has a patent method for lipoprotein characterization licensed to Biosfer Teslab (Spain), of which she is a stock owner, a company that commercializes the lipoprotein and glycoprotein profiles described in the present manuscript. The funders had no role in study design, data analysis, interpretation, or decision to publish.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
