

Recent Advances in Pathophysiology and Management of Transient Tachypnea of Newborn
- PMID: 32753712
- PMCID: PMC11867197
- DOI: 10.1038/s41372-020-0757-3
Recent Advances in Pathophysiology and Management of Transient Tachypnea of Newborn
Abstract
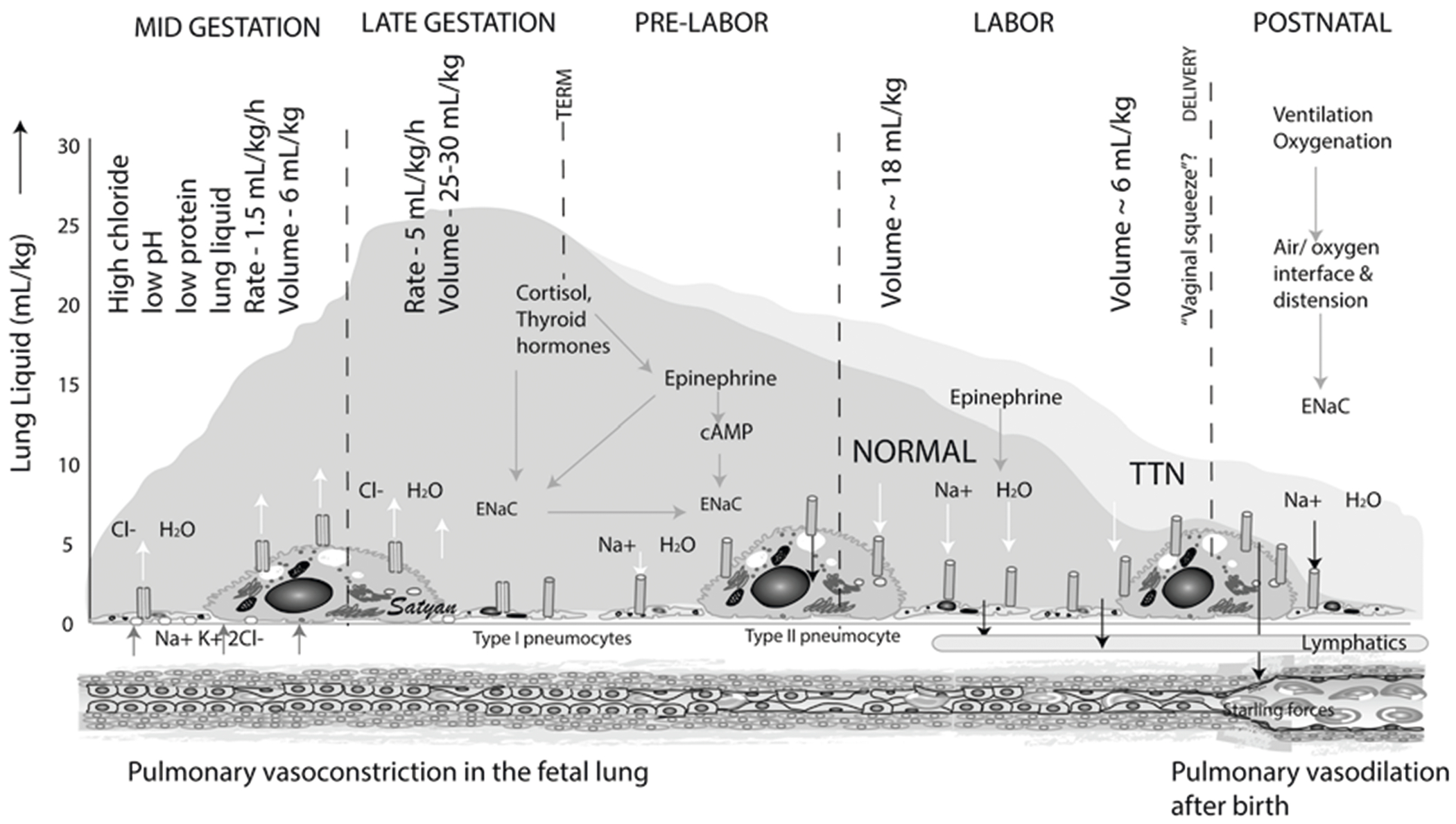
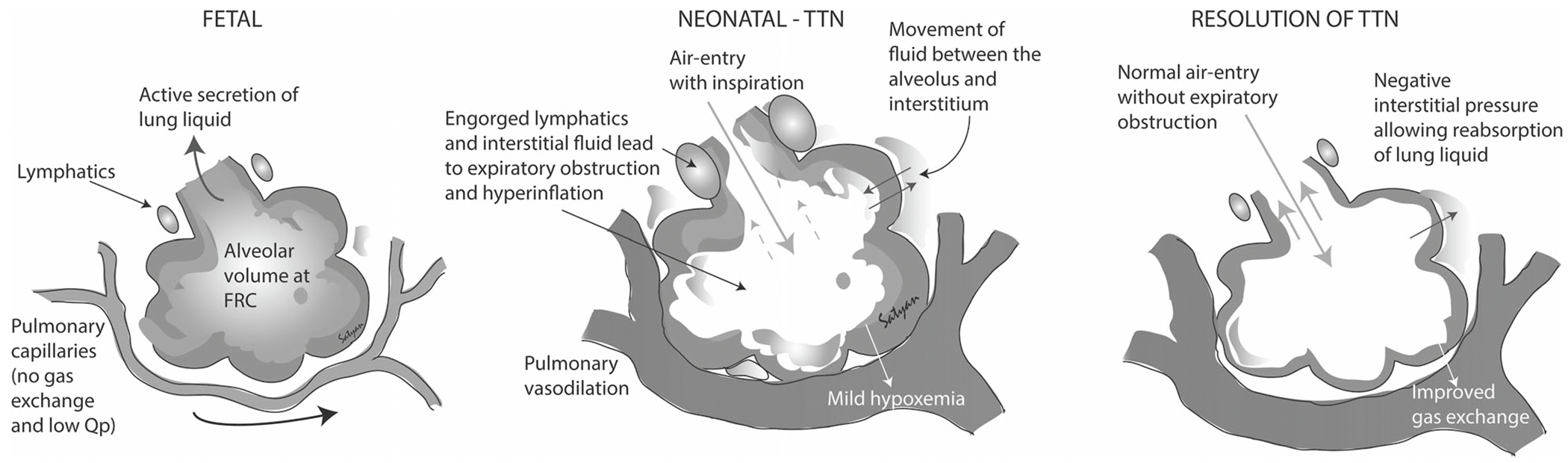
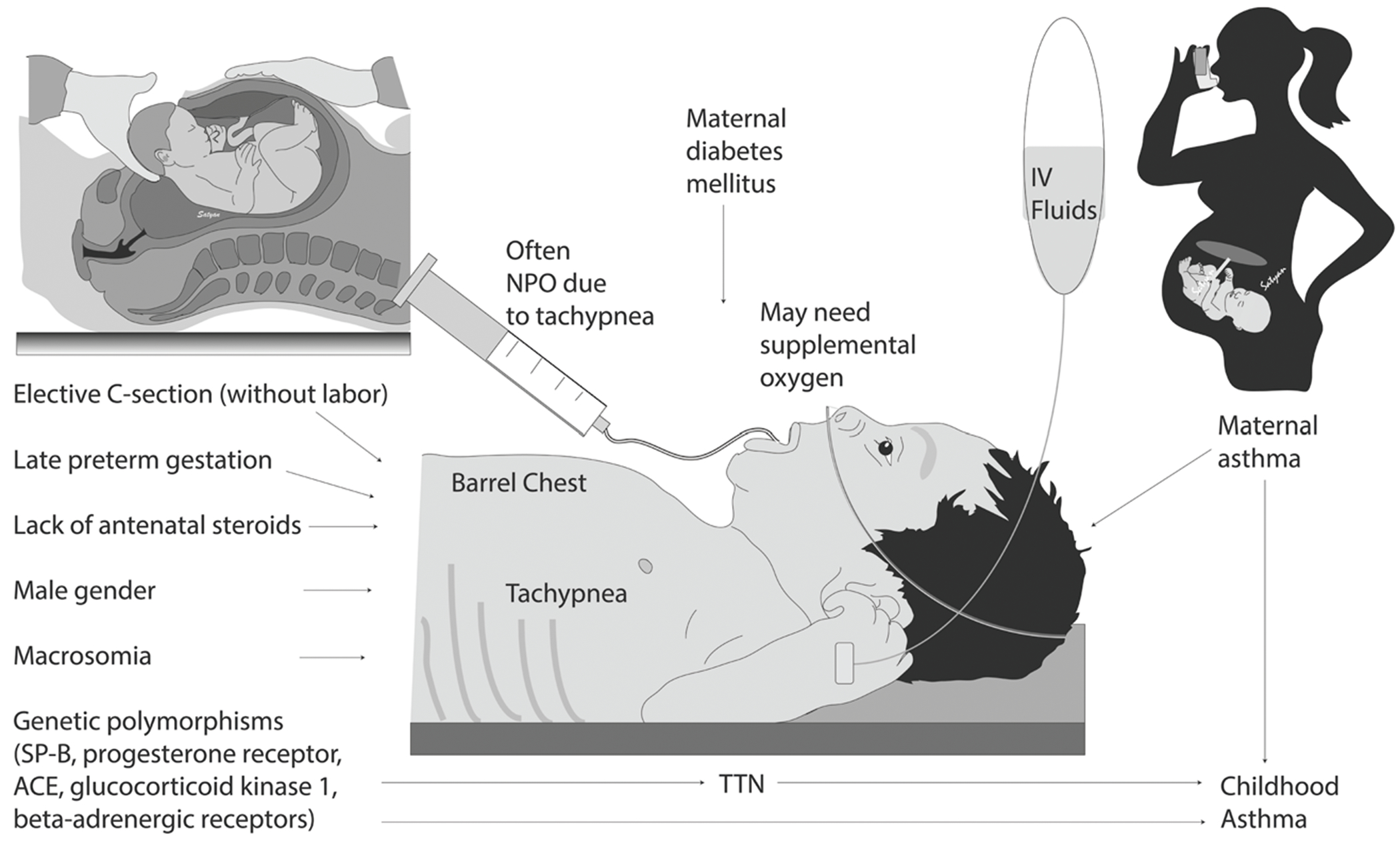
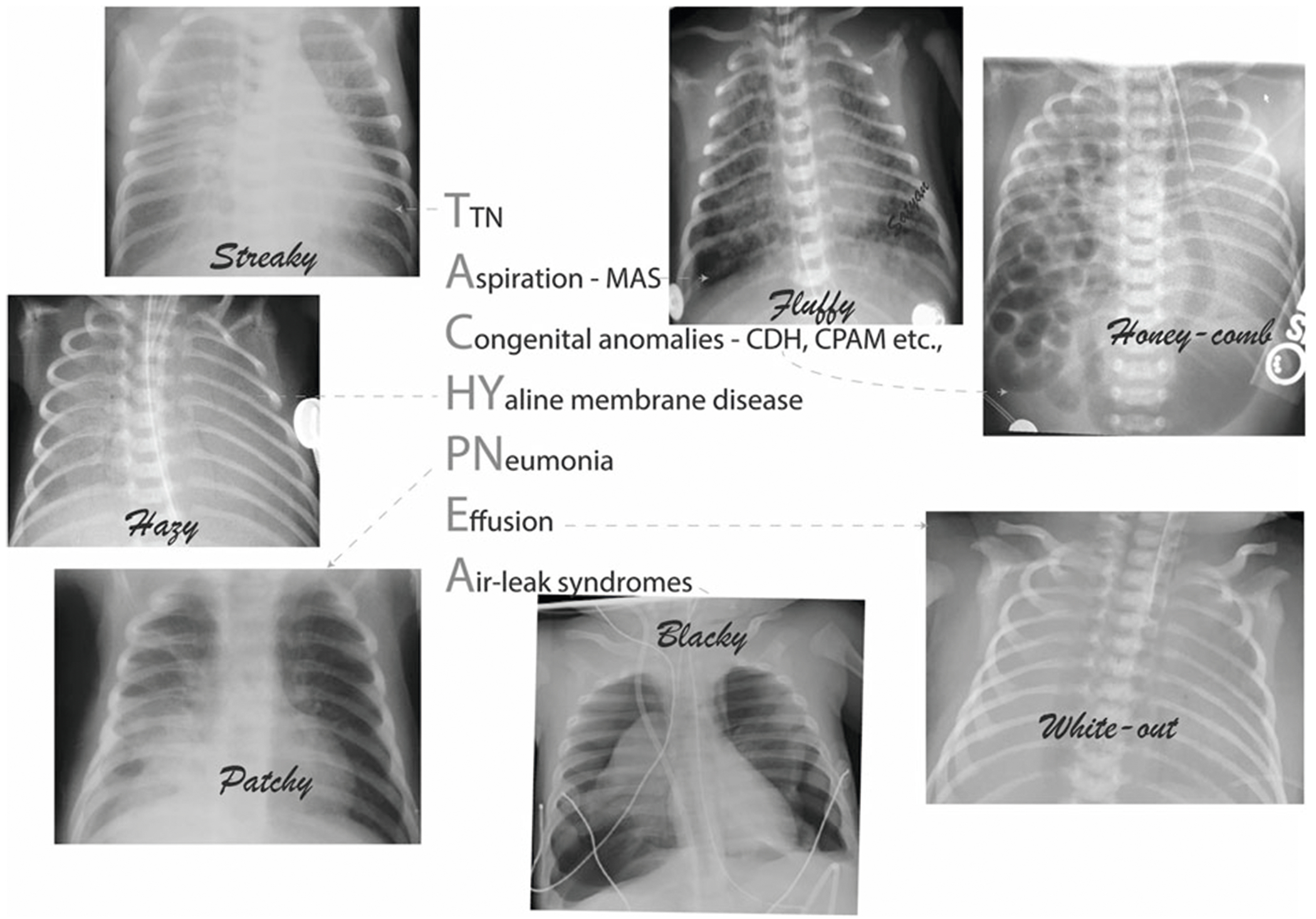
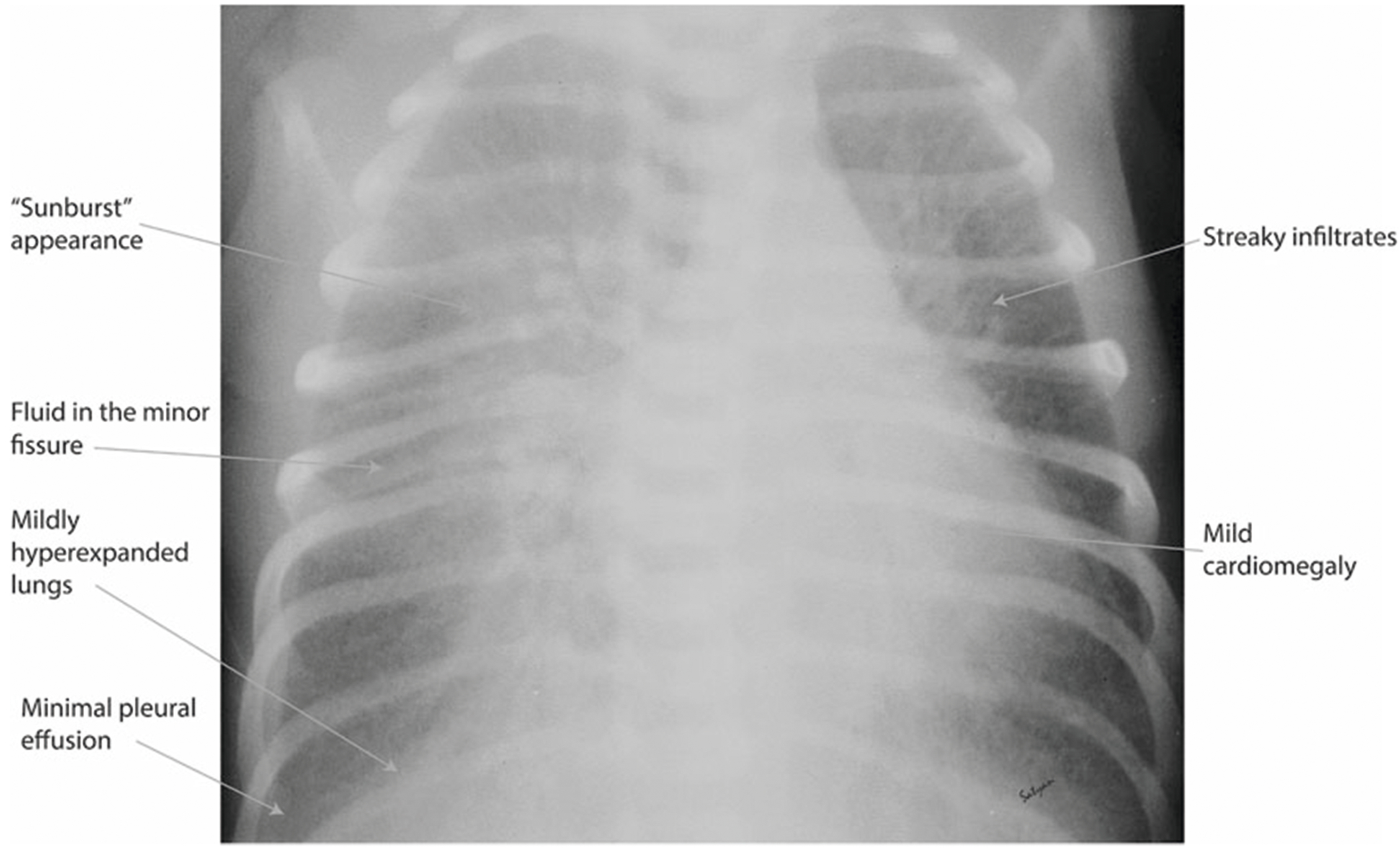
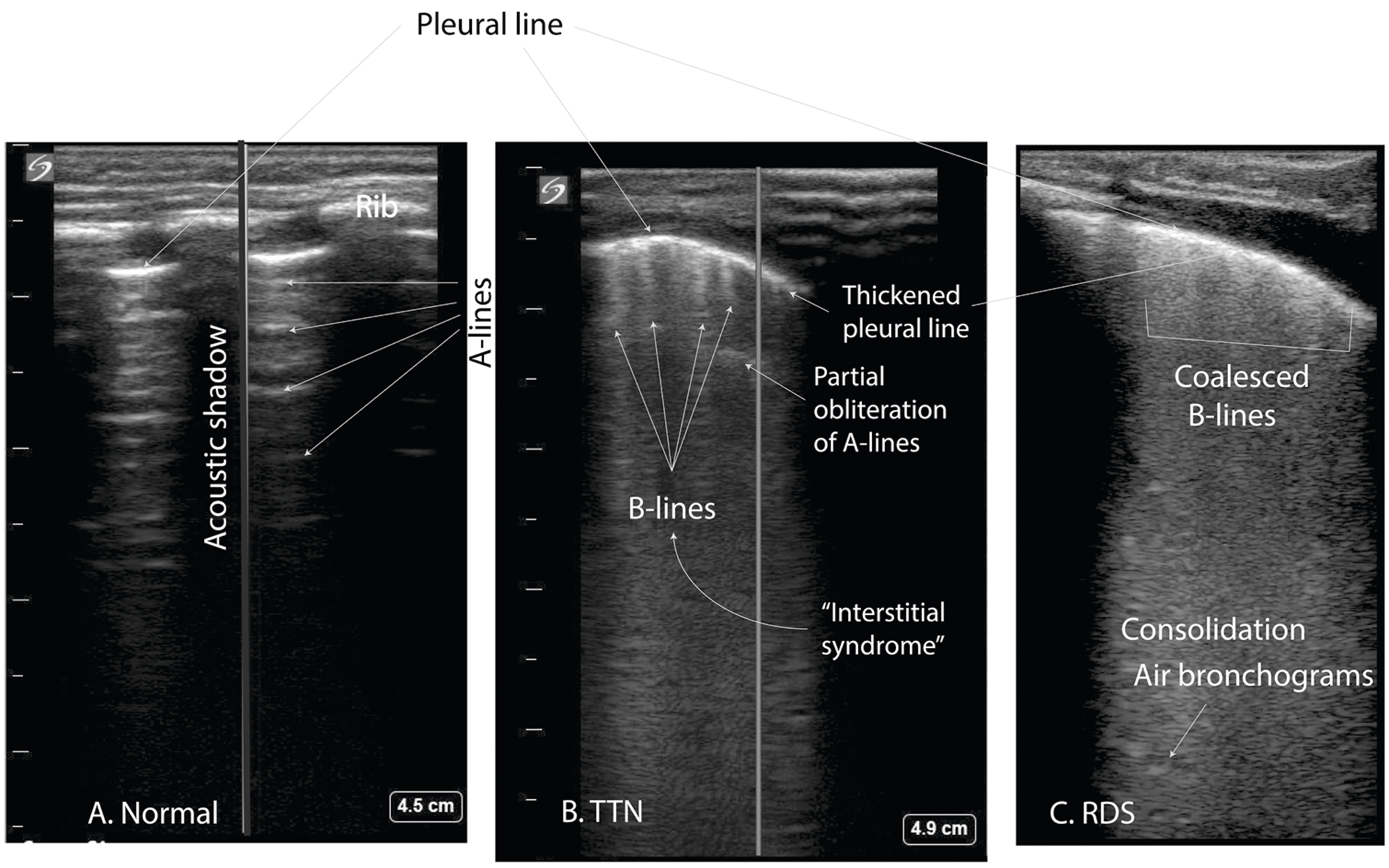
Transient tachypnea of newborn (TTN) results from failure of the newborn to effectively clear the fetal lung fluid soon after birth. TTN represents the most common etiology of respiratory distress in term gestation newborns and sometimes requires admission to the neonatal intensive care unit. TTN can lead to maternal-infant separation, the need for respiratory support, extended unnecessary exposure to antibiotics and prolonged hospital stays. Recent evidence also suggests that TTN may be associated with wheezing syndromes later in childhood. New imaging modalities such as lung ultrasound can help in the diagnosis of TTN and early management with distending pressure using continuous positive airway pressure may prevent exacerbation of respiratory distress.
Conflict of interest statement
PV is supported by NIH grant (1R03HD09299-01). SL is supported by NIH grant (5R01HD072929-08). ZA, LG, and RMR have no financial relationships to disclose relevant to this article. This commentary does not contain a discussion of an unapproved/investigative use of a commercial product/device. The use of antenatal betamethasone, diuretics and beta-agonists are not approved by the FDA in the prevention or treatment of TTN.
Figures
References
-
- Guglani L, Lakshminrusimha S, Ryan RM. Transient tachypnea of the newborn. Pediatr Rev. 2008;29:e59–65. - PubMed
-
- Jain L. Alveolar fluid clearance in developing lungs and its role in neonatal transition. Clin Perinatol. 1999;26:585–99. - PubMed
-
- Zanardo V, Simbi AK, Franzoi M, Solda G, Salvadori A, Trevisanuto D. Neonatal respiratory morbidity risk and mode of delivery at term: influence of timing of elective caesarean delivery. Acta Paediatr. 2004;93:643–7. - PubMed
-
- Jost A, Policard A. Contribution experimentale à l’étude du développment prenatal du poumon chez le lapin. Arch Anat Micr. 1948;37:327–32.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
