Spheno-Orbital Meningiomas: Optimizing Visual Outcome
- PMID: 32753802
- PMCID: PMC7394617
- DOI: 10.1055/s-0040-1709270
Spheno-Orbital Meningiomas: Optimizing Visual Outcome
Abstract
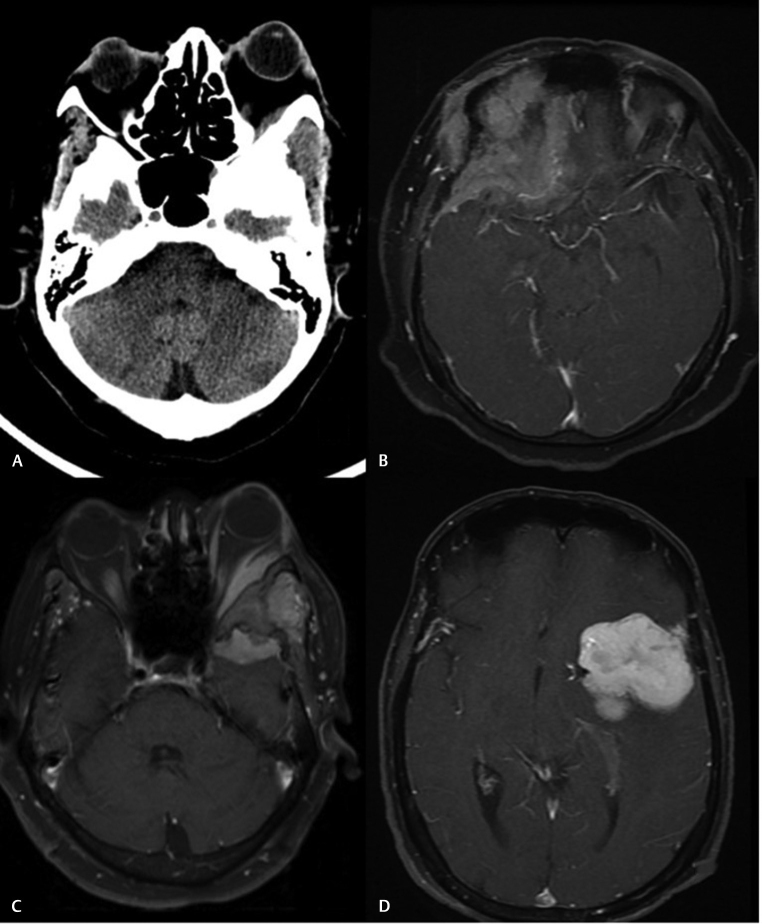
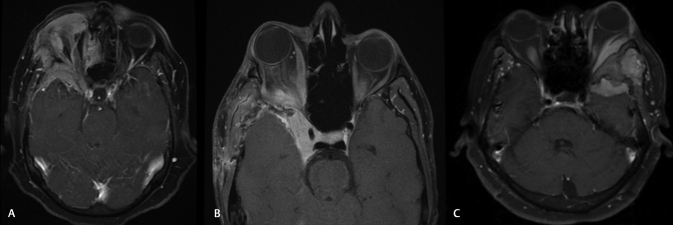
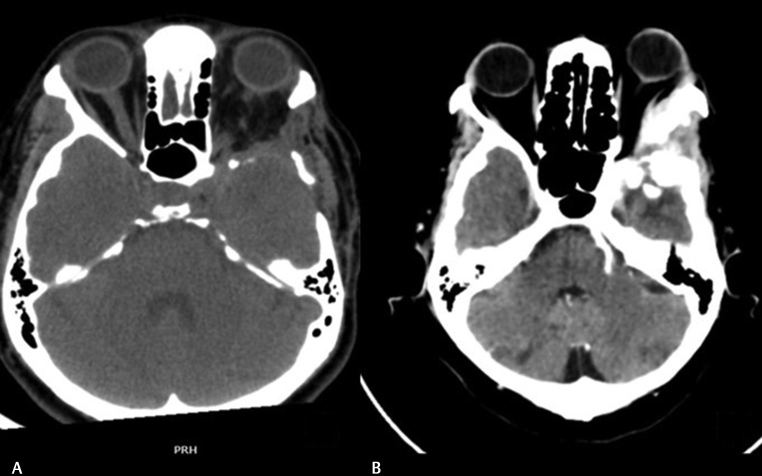
Background Spheno-orbital meningiomas (SOMs) constitute a rare cause for orbital proptosis and visual impairment. This study aims to share our outcome experience with regard to vision and exophthalmos following the surgical management of 17 patients with SOM. Methods Retrospective analysis of the case records of all surgically treated SOMs in the last 10 years. Exophthalmos index (EI) was calculated based on preoperative magnetic resonance imaging/computed tomography imaging. Vision was assessed using the Snellen's chart and Goldman's perimeter. Orbital volume was calculated using three-dimensional volume rendering assisted region-of-interest computation. Preoperative duration of symptoms and extent of surgery were the other predictors analyzed. Results Patients' age ranged from 17 to 72 years (mean, 50.57 y; median, 50.0 years). Women represented 13 (76.4%) of the entire study group. Proptosis (14/17; 82.4%) and visual impairment (14/17; 82.3%) were the two most common presenting complaints followed by headache (12/17; 70.1%). Gross total resection (GTR) was achieved in only 2 of the 17 patients (11.8%). Majority of the tumors were benign World Health Organization Grade I meningiomas (14/17; 84%). Mean follow-up time for the entire cohort was 56 months. Postoperatively, proptosis improved in nine (64.3%) and remained static in the rest five (35.7%) of patients. Four patients (28.6%) improved in vision following surgery. Vision remained static in eight patients (57.1%). Vision deteriorated in two (14.3%) patients who had severe preoperative visual deficits. New onset oculomotor palsy, trigeminal dysfunction, and mechanical ocular motility restriction were noticed in three (17.6%), two (11.2%), and six (35.3%) patients, respectively. The mean preoperative orbital volume was 21.68 ± 3.2 cm 3 and the mean postoperative orbital volume was 23.72 ± 3.4 cm 3 . Orbital volume was inversely related to EI. Optic canal (OC) deroofing and extensive orbital wall decompression facilitated visual improvement and proptosis reduction. None of the variables including orbital volume proved to be statistically significant in predicting outcome. Conclusion SOMs constitute a rare subgroup of skull base meningiomas that pose considerable surgical challenges. A surgical strategy aimed at safe maximal resection rather than aggressive GTR provides favorable outcome with less morbidity. Adequate bony decompression of the orbital walls and OC provides satisfactory improvements in proptosis and vision. Residual disease is common, but the risk of symptomatic recurrence is low especially when combined with adjuvant radiotherapy. Visual outcome is likely to be poor in patients presenting with severely compromised vision.
Keywords: exophthalmos; meningiomas; optic; orbit; sphenoid.
Conflict of interest statement
Conflict of Interest None declared.
Figures
References
-
- Bikmaz K, Mrak R, Al-Mefty O. Management of bone-invasive, hyperostotic sphenoid wing meningiomas. J Neurosurg. 2007;107(05):905–912. - PubMed
-
- Gonen L, Nov E, Shimony N, Shofty B, Margalit N. Sphenoorbital meningioma: surgical series and design of an intraoperative management algorithm. Neurosurg Rev. 2018;41(01):291–301. - PubMed
-
- Scarone P, Leclerq D, Héran F, Robert G. Long-term results with exophthalmos in a surgical series of 30 sphenoorbital meningiomas. Clinical article. J Neurosurg. 2009;111(05):1069–1077. - PubMed
-
- Schick U, Bleyen J, Bani A, Hassler W. Management of meningiomas en plaque of the sphenoid wing. J Neurosurg. 2006;104(02):208–214. - PubMed
-
- Boari N, Gagliardi F, Spina A, Bailo M, Franzin A, Mortini P. Management of spheno-orbital en plaque meningiomas: clinical outcome in a consecutive series of 40 patients. Br J Neurosurg. 2013;27(01):84–90. - PubMed