

Using Deep Learning to Accelerate Knee MRI at 3 T: Results of an Interchangeability Study
- PMID: 32755163
- PMCID: PMC8209682
- DOI: 10.2214/AJR.20.23313
Using Deep Learning to Accelerate Knee MRI at 3 T: Results of an Interchangeability Study
Abstract
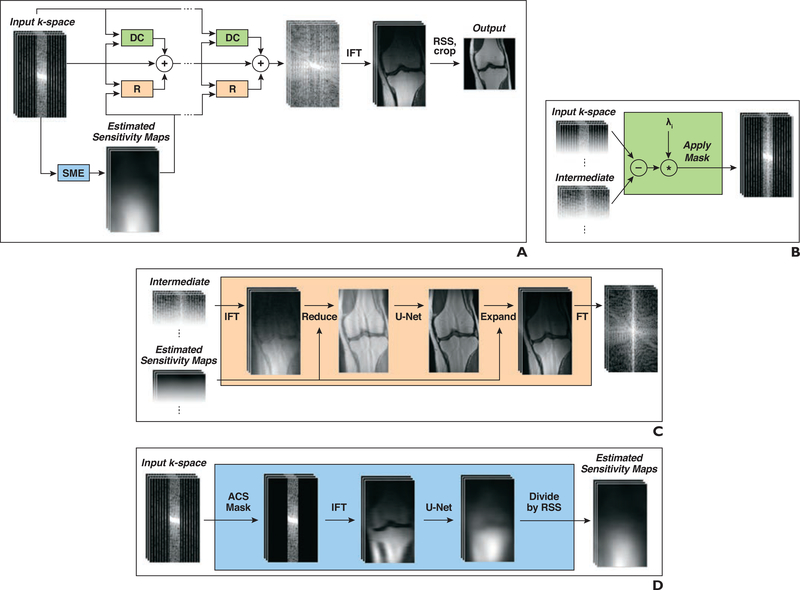
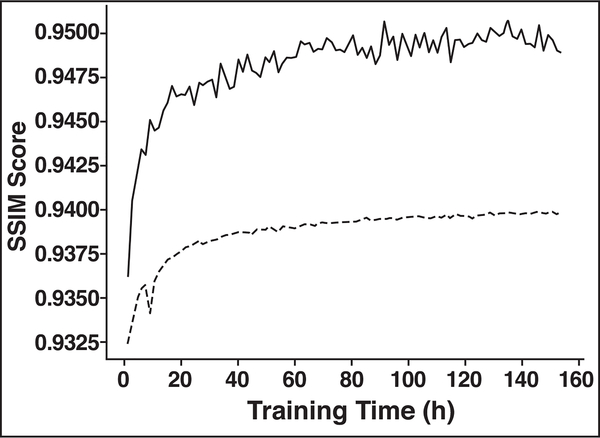
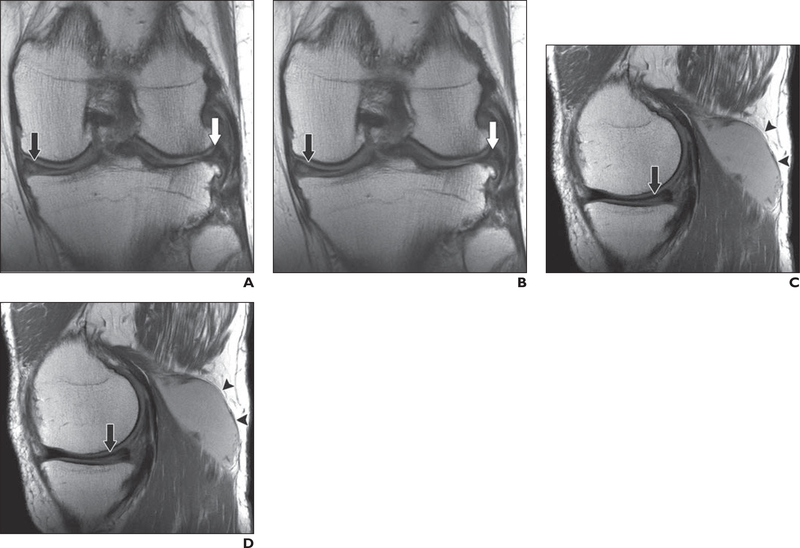
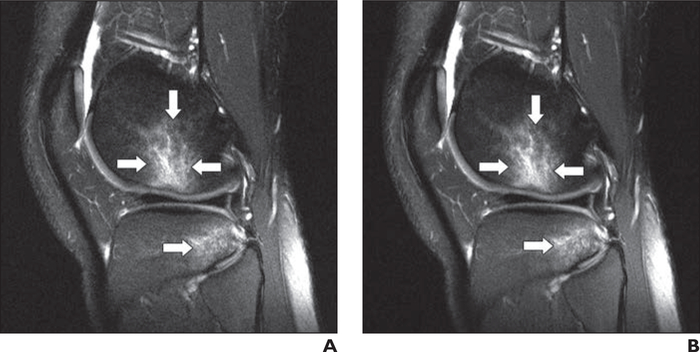
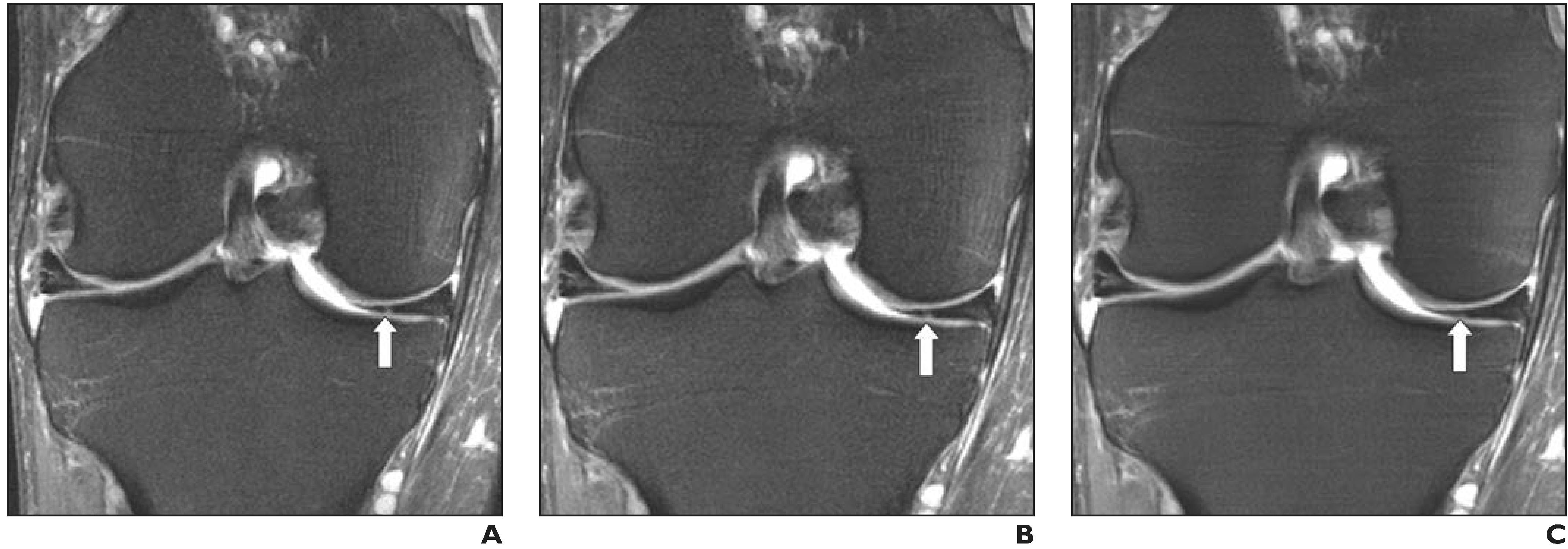
OBJECTIVE. Deep learning (DL) image reconstruction has the potential to disrupt the current state of MRI by significantly decreasing the time required for MRI examinations. Our goal was to use DL to accelerate MRI to allow a 5-minute comprehensive examination of the knee without compromising image quality or diagnostic accuracy. MATERIALS AND METHODS. A DL model for image reconstruction using a variational network was optimized. The model was trained using dedicated multisequence training, in which a single reconstruction model was trained with data from multiple sequences with different contrast and orientations. After training, data from 108 patients were retrospectively undersampled in a manner that would correspond with a net 3.49-fold acceleration of fully sampled data acquisition and a 1.88-fold acceleration compared with our standard twofold accelerated parallel acquisition. An interchangeability study was performed, in which the ability of six readers to detect internal derangement of the knee was compared for clinical and DL-accelerated images. RESULTS. We found a high degree of interchangeability between standard and DL-accelerated images. In particular, results showed that interchanging the sequences would produce discordant clinical opinions no more than 4% of the time for any feature evaluated. Moreover, the accelerated sequence was judged by all six readers to have better quality than the clinical sequence. CONCLUSION. An optimized DL model allowed acceleration of knee images that performed interchangeably with standard images for detection of internal derangement of the knee. Importantly, readers preferred the quality of accelerated images to that of standard clinical images.
Keywords: MRI; acceleration; deep learning; internal derangement; knee.
Figures

References
-
- Gielen JL, De Schepper AM, Vanhoenacker F, et al. Accuracy of MRI in characterization of soft tissue tumors and tumor-like lesions: a prospective study in 548 patients. Eur Radiol 2004; 14:2320–2330 - PubMed
-
- Vahey TN, Meyer SF, Shelbourne KD, Klootwyk TE. MR imaging of anterior cruciate ligament injuries. Magn Reson Imaging Clin N Am 1994; 2:365–380 - PubMed
-
- Floriani I, Torri V, Rulli E, et al. Performance of imaging modalities in diagnosis of liver metastases from colorectal cancer: a systematic review and meta-analysis. J Magn Reson Imaging 2010; 31:19–31 - PubMed
-
- Martín Noguerol T, Barousse R, Gómez Cabrera M, Socolovsky M, Bencardino JT, Luna A. Functional MR neurography in evaluation of peripheral nerve trauma and postsurgical assessment. RadioGraphics 2019; 39:427–446 - PubMed
-
- Vanderby S, Badea A, Peña Sánchez JN, Kalra N, Babyn P. Variations in magnetic resonance imaging provision and processes among Canadian academic centres. Can Assoc Radiol J 2017; 68:56–65 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
