

Multicenter Multireader Evaluation of an Artificial Intelligence-Based Attention Mapping System for the Detection of Prostate Cancer With Multiparametric MRI
- PMID: 32755355
- PMCID: PMC8974983
- DOI: 10.2214/AJR.19.22573
Multicenter Multireader Evaluation of an Artificial Intelligence-Based Attention Mapping System for the Detection of Prostate Cancer With Multiparametric MRI
Abstract
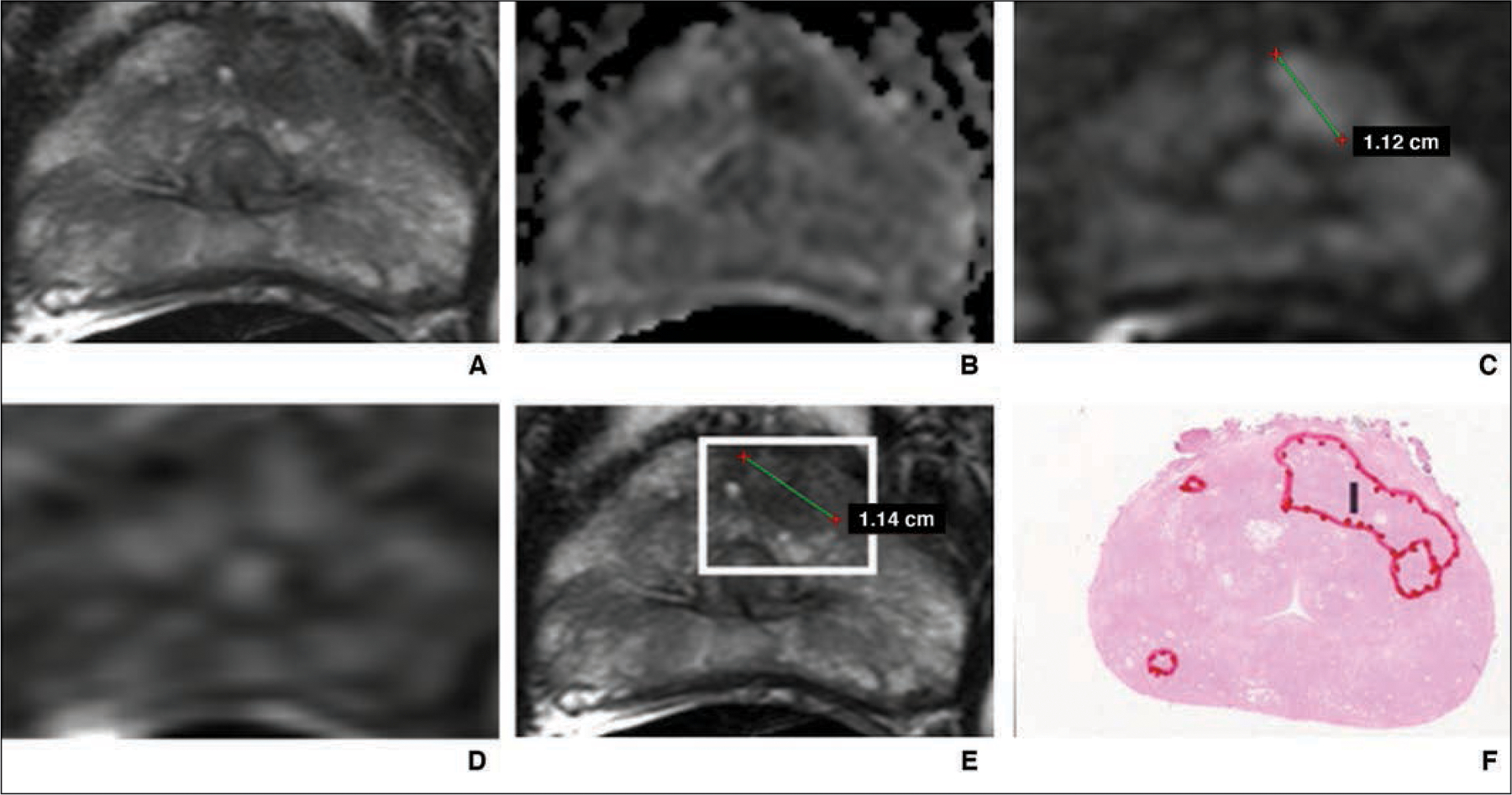
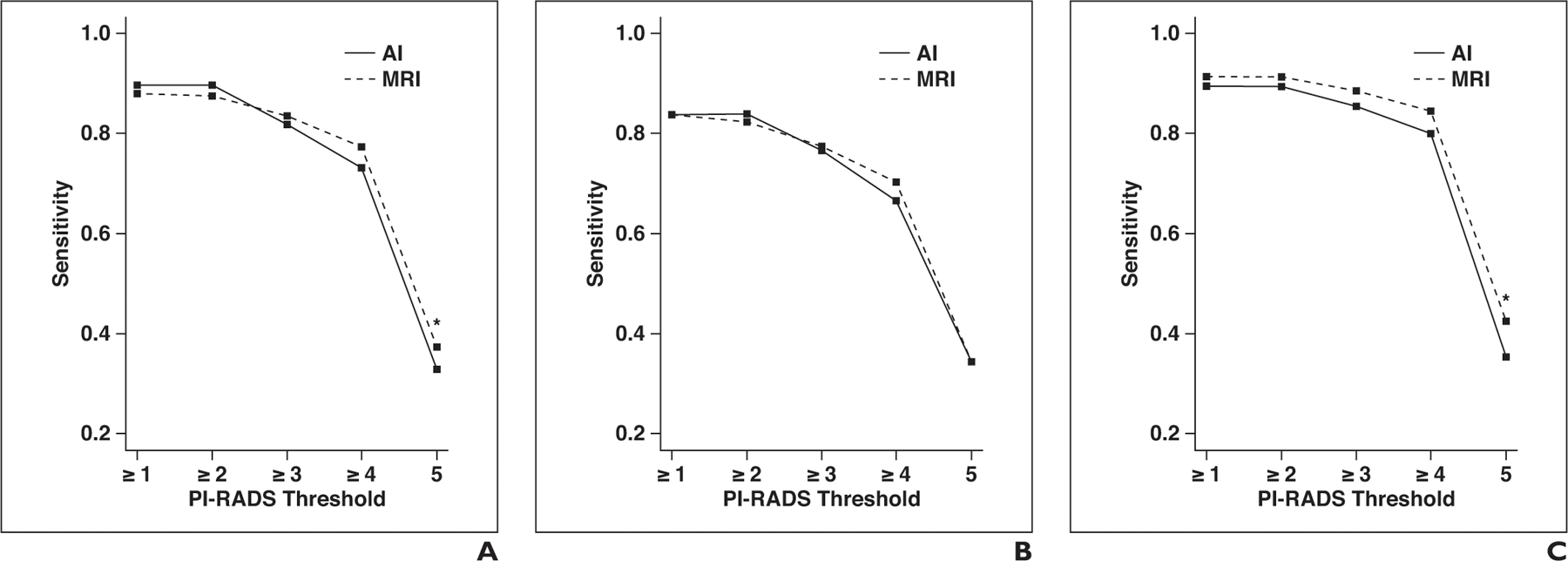
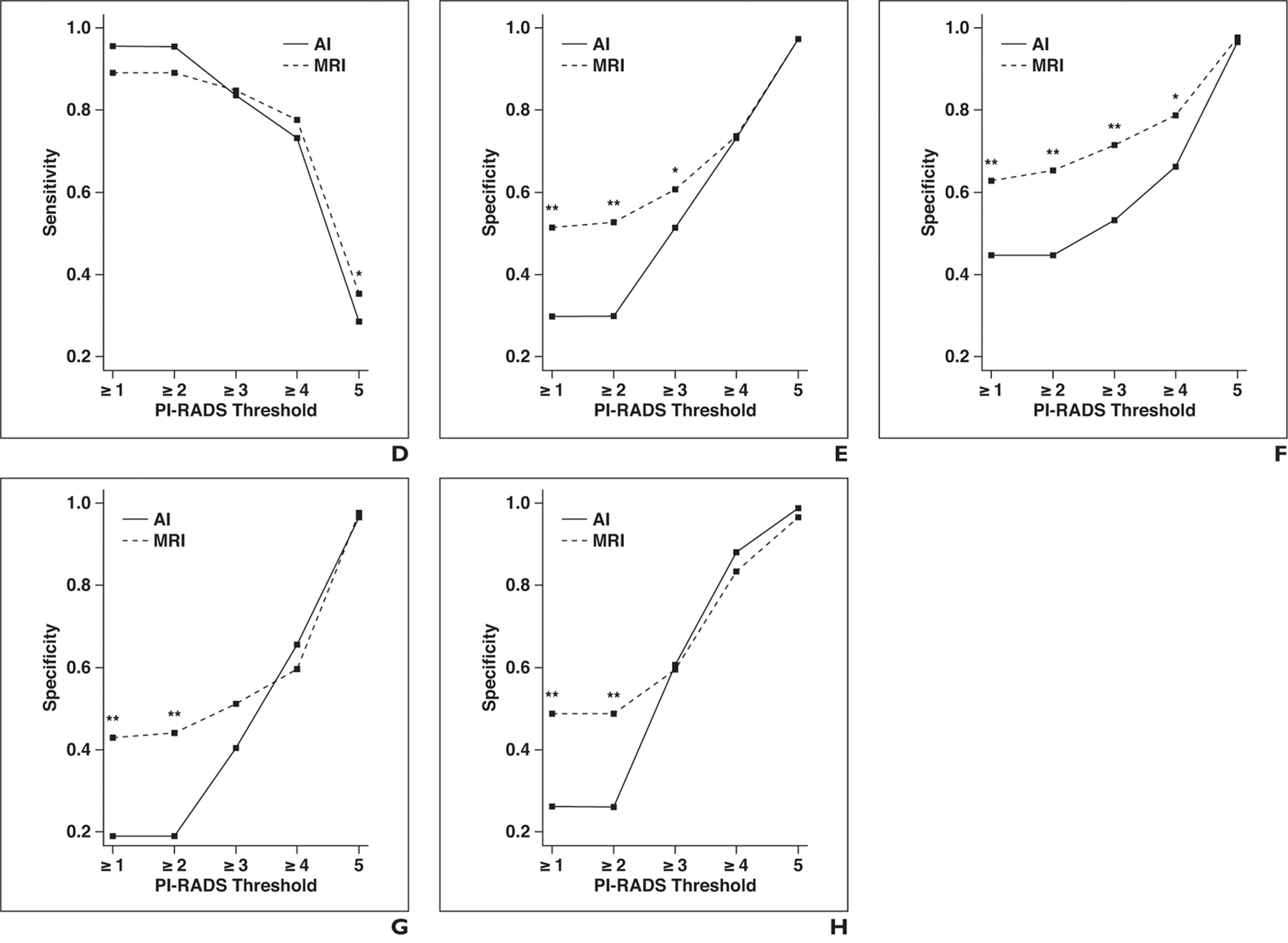
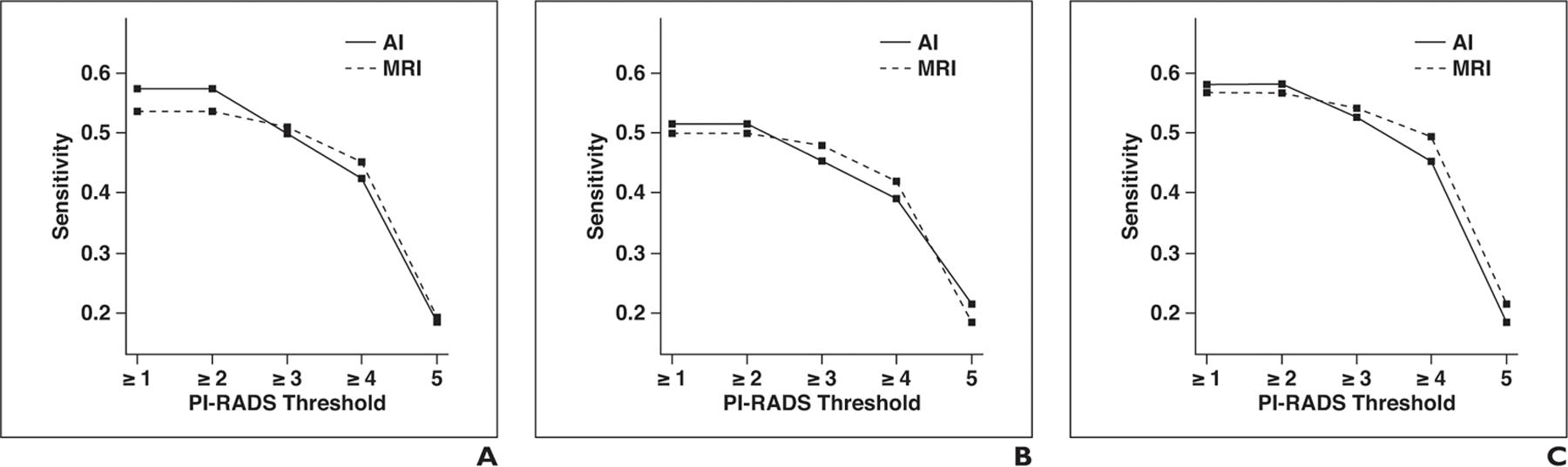
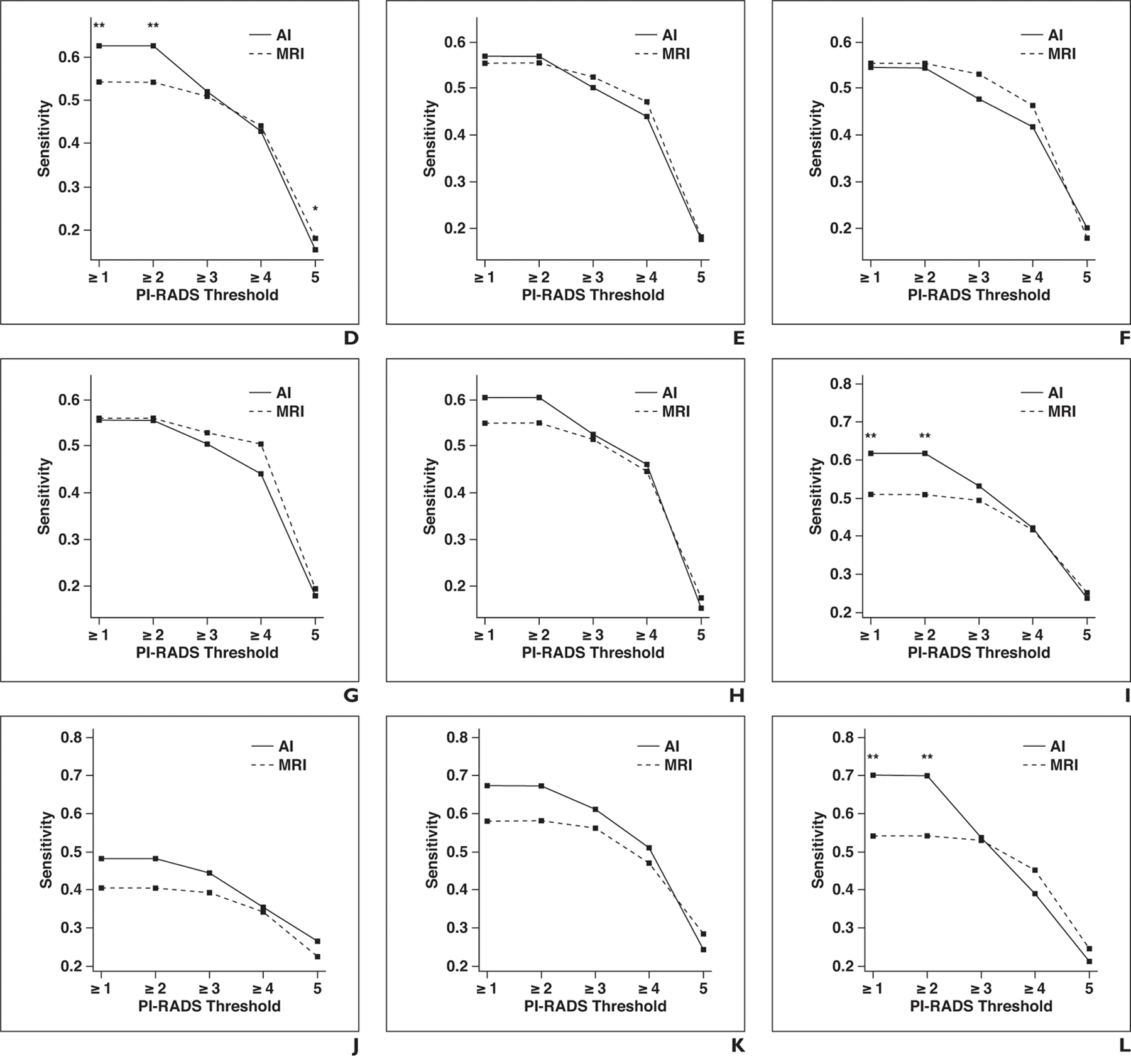
OBJECTIVE. The purpose of this study was to evaluate in a multicenter dataset the performance of an artificial intelligence (AI) detection system with attention mapping compared with multiparametric MRI (mpMRI) interpretation in the detection of prostate cancer. MATERIALS AND METHODS. MRI examinations from five institutions were included in this study and were evaluated by nine readers. In the first round, readers evaluated mpMRI studies using the Prostate Imaging Reporting and Data System version 2. After 4 weeks, images were again presented to readers along with the AI-based detection system output. Readers accepted or rejected lesions within four AI-generated attention map boxes. Additional lesions outside of boxes were excluded from detection and categorization. The performances of readers using the mpMRI-only and AI-assisted approaches were compared. RESULTS. The study population included 152 case patients and 84 control patients with 274 pathologically proven cancer lesions. The lesion-based AUC was 74.9% for MRI and 77.5% for AI with no significant difference (p = 0.095). The sensitivity for overall detection of cancer lesions was higher for AI than for mpMRI but did not reach statistical significance (57.4% vs 53.6%, p = 0.073). However, for transition zone lesions, sensitivity was higher for AI than for MRI (61.8% vs 50.8%, p = 0.001). Reading time was longer for AI than for MRI (4.66 vs 4.03 minutes, p < 0.001). There was moderate interreader agreement for AI and MRI with no significant difference (58.7% vs 58.5%, p = 0.966). CONCLUSION. Overall sensitivity was only minimally improved by use of the AI system. Significant improvement was achieved, however, in the detection of transition zone lesions with use of the AI system at the cost of a mean of 40 seconds of additional reading time.
Keywords: MRI; artificial intelligence; laparoscopic; multiparametric; prostate cancer; radical prostatectomy; robot-assisted.
Figures
Comment in
-
Urological Oncology: Prostate Cancer.J Urol. 2021 Jan;205(1):303-306. doi: 10.1097/JU.0000000000001472. Epub 2020 Nov 12. J Urol. 2021. PMID: 33179582 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68:7–30 - PubMed
-
- Hricak H, Williams RD, Spring DB, et al. Anatomy and pathology of the male pelvis by magnetic resonance imaging. AJR 1983; 141:1101–1110 - PubMed
-
- Hamoen EHJ, de Rooij M, Witjes JA, Barentsz JO, Rovers MM. Use of the Prostate Imaging Reporting and Data System (PI-RADS) for prostate cancer detection with multiparametric magnetic resonance imaging: a diagnostic meta-analysis. Eur Urol 2015; 67:1112–1121 - PubMed
-
- Le JD, Tan N, Shkolyar E, et al. Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: correlation with whole-mount histopathology. Eur Urol 2015; 67:569–576 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
