

Study on preventing adverse events in neonates (SEPREVEN): A stepped-wedge randomised controlled trial to reduce adverse event rates in the NICU
- PMID: 32756081
- PMCID: PMC7402760
- DOI: 10.1097/MD.0000000000020912
Study on preventing adverse events in neonates (SEPREVEN): A stepped-wedge randomised controlled trial to reduce adverse event rates in the NICU
Abstract
Introduction: Adverse events (AE) in care are recognized as a leading cause of mortality and injury in patients. Improving patients' safety is difficult to achieve. Therefore, innovative research strategies are needed to identify errors in subgroups of patients and related severity of outcomes as well as reliably measured efficiency of reproducible strategies to improve safety. This trial aims to evaluate the impact of a combined multiprofessional education program on the rate of AE in neonatal intensive care units (NICUs).
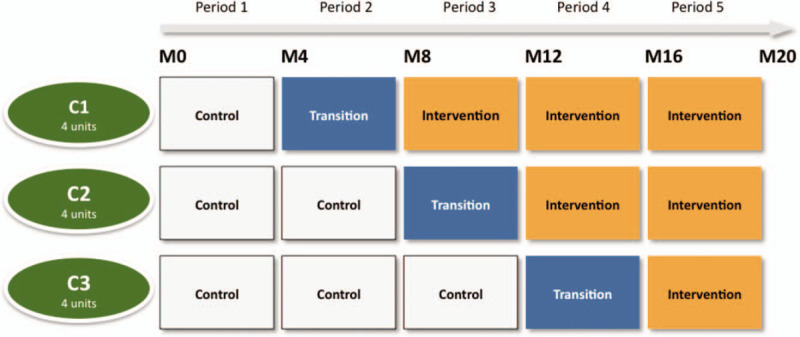
Methods and analysis: This is a stepped-wedge cluster randomised controlled trial with 3 clusters each containing 4 units. The study time period will be 20 months. The education program will be implemented within each cluster following a random sequence with a control period, a 4-month transition period and a post-educational intervention period. Eligibility criteria: for clusters: 6 NICUs from Ile-de-France and 6 NICUs from different regions in France; for patients: in-hospital during the study period (November 23, 2015 and November 2, 2017 [inclusion start dates varying by unit]) in one of the 12 NICUs; corrected gestational age ≤42 weeks upon admission; hospitalization period >2 days; and parents informed and not opposed to the use of their newborn's data. A routine occurrence reporting of medical errors and their consequence will take place during the entire study period. The intervention will combine an education to implement a standardized root cause analysis method, creation of bundles (insertion, daily goals, maintenance bundles) to prevent catheter-associated blood-stream infection and a poster to prevent extravasation injuries.
Outcome: We hypothesize a reduction from 60 (control) to 50 (intervention) AE/1000 patient-days. The primary outcome will be the rate of AE/1000 patient-days in the NICU.
Trial registration number: NCT02598609, trial registered November 6, 2015. https://clinicaltrials.gov/ct2/show/NCT02598609.
Ethics and dissemination: Study approved by the regional ethic committee CPP Ile-de-France III (no 2014-A01751-46). The results will be published in peer-reviewed journals.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kohn LT, Corrigan JM, Donaldson MS. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999. - PubMed
-
- Makary MA, Daniel M. Medical error — the third leading cause of death in the US. BMJ 2016;353:i2139.doi: 10.1136/bmj.i2139. - PubMed
-
- Leape LL. Error in medicine. JAMA 1994;272:1851–7. [published Online First: 1994/12/21]. - PubMed
-
- Reason J. Human Error. Cambridge: Cambridge University Press; 1990.
-
- Landrigan CP, Parry GJ, Bones CB, et al. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med 2010;363:2124–34. doi: 10.1056/NEJMsa1004404 [published Online First: 2010/11/26]. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
