

Laryngeal Movement Disorders in Multiple System Atrophy: A Diagnostic Biomarker?
- PMID: 32757231
- PMCID: PMC7818263
- DOI: 10.1002/mds.28220
Laryngeal Movement Disorders in Multiple System Atrophy: A Diagnostic Biomarker?
Abstract
Background: Multiple system atrophy (MSA) is a rare neurodegenerative disorder, and its parkinsonian variant can be difficult to delineate from Parkinson's disease (PD). Despite laryngeal dysfunction being associated with decreased life expectancy and quality of life, systematic assessments of laryngeal dysfunction in large cohorts are missing.
Objectives: The objective of this study was to systematically assess laryngeal dysfunction in MSA and PD and identify laryngeal symptoms that allow for differentiating MSA from PD.
Methods: Patients with probable or possible MSA underwent flexible endoscopic evaluation of swallowing performing a systematic task protocol. Findings were compared with an age-matched PD cohort.
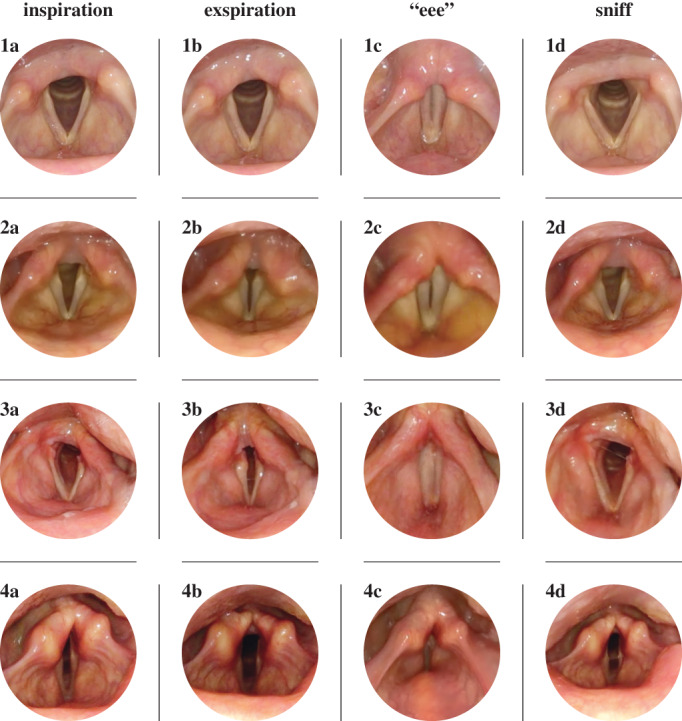
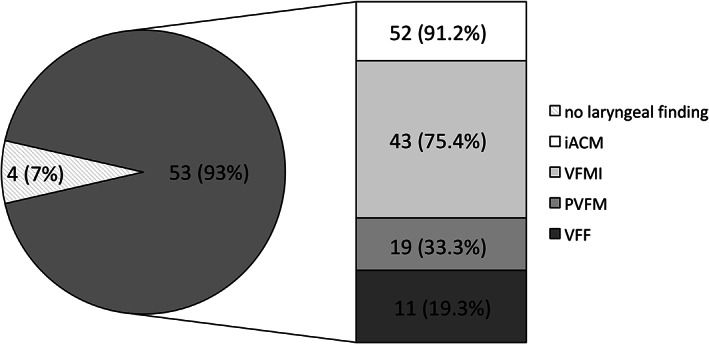
Results: A total of 57 patients with MSA (64 [59-71] years; 35 women) were included, and task assessments during endoscopic examination compared with 57 patients with PD (67 [60-73]; 28 women). Patients with MSA had a shorter disease duration (4 [3-5] years vs 7 [5-10]; P < 0.0001) and higher disease severity (Hoehn & Yahr stage 4 [3-4] vs 3 [2-4]; P < 0.0001). Of the patients with MSA, 43.9% showed clinically overt laryngeal dysfunction with inspiratory stridor. During endoscopic task assessment, however, 93% of patients with MSA demonstrated laryngeal dysfunction in contrast with only 1.8% of patients with PD (P < 0.0001). Irregular arytenoid cartilages movements were present in 91.2% of patients with MSA, but in no patients with PD (P < 0.0001). Further findings included vocal fold motion impairment (75.4%), paradoxical vocal fold motion (33.3%), and vocal fold fixation (19.3%). One patient with PD showed vocal fold motion impairment.
Conclusion: Laryngeal movement disorders are highly prevalent in patients with MSA when assessed by a specific task protocol despite the lack of overt clinical symptoms. Our data suggest that irregular arytenoid cartilage movements could be used as a clinical marker to delineate MSA from PD with a specificity of 1.0 and sensitivity 0.9. © 2020 The Authors. Movement Disorders published by Wiley Periodicals LLC on behalf of International Parkinson and Movement Disorder Society.
Keywords: FEES; differential diagnosis; irregular arytenoid cartilages movements; larynx; multiple system atrophy.
© 2020 The Authors. Movement Disorders published by Wiley Periodicals LLC on behalf of International Parkinson and Movement Disorder Society.
Figures
Comment in
-
Reply to: "Laryngeal Movement Disorders in Multiple System Atrophy: A Diagnostic Biomarker?".Mov Disord. 2021 Aug;36(8):2000-2001. doi: 10.1002/mds.28694. Mov Disord. 2021. PMID: 34409689 No abstract available.
-
Reply to: "Laryngeal Movement Disorders in Multiple System Atrophy: A Diagnostic Biomarker?".Mov Disord. 2021 Aug;36(8):1999-2000. doi: 10.1002/mds.28697. Mov Disord. 2021. PMID: 34409690 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
