

Non-Motor Symptoms in Parkinson's Disease are Reduced by Nabilone
- PMID: 32757413
- PMCID: PMC7540547
- DOI: 10.1002/ana.25864
Non-Motor Symptoms in Parkinson's Disease are Reduced by Nabilone
Abstract
Objective: The objective of this study was to assess the efficacy and safety of nabilone, a synthetic tetrahydrocannabinol analogue, as a treatment for non-motor symptoms (NMS) in Parkinson's disease (PD).
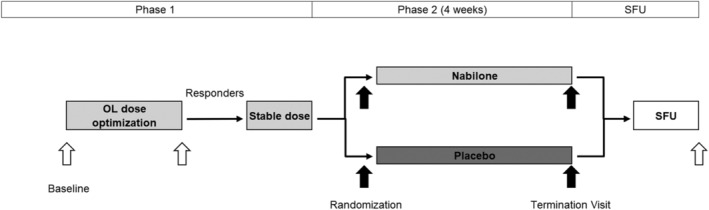
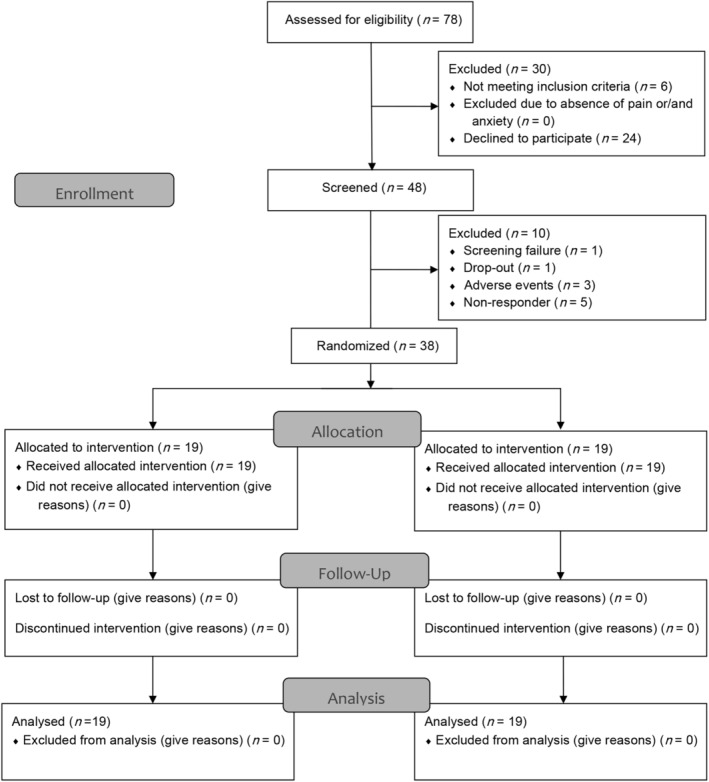
Methods: This was a phase II placebo-controlled, double-blind, parallel-group, enriched enrollment randomized withdrawal trial conducted at the Medical University Innsbruck. A random sample of 47 patients with PD with stable motor disease and disturbing NMS defined by a score of ≥4 points on the Movement Disorder Society - Unified PD Rating Scale-I (MDS-UPDRS-I) underwent open-label nabilone titration (0.25 mg once daily to 1 mg twice daily, phase I). Responders were randomized 1:1 to continue with nabilone or switch to placebo for 4 weeks (phase II). The primary efficacy criterion was the change of the MDS-UPDRS-I between randomization and week 4. Safety was analyzed in all patients who received at least one nabilone dose.
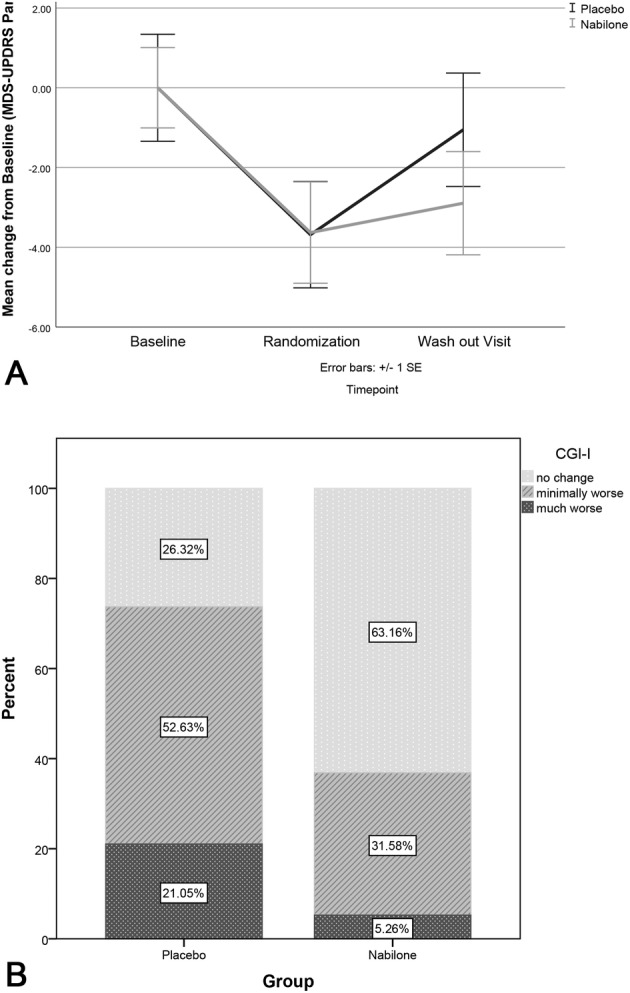
Results: Between October 2017 and July 2019, 19 patients received either nabilone (median dose = 0.75 mg) or placebo. At week 4, mean change of the MDS-UPDRS-I was 2.63 (95% confidence interval [CI] 1.53 to 3.74, p = 0.002, effect size = 1.15) in the placebo versus 1.00 (95% CI -0.16 to 2.16, p = 0.280, effect size = 0.42) in the nabilone-group (difference: 1.63, 95% CI 0.09 to 3.18, p = 0.030, effect size = 0.66). Seventy-seven percent of patients had adverse events (AEs) during open-label titration, most of them were transient. In the double-blind phase, similar proportions of patients in each group had AEs (42% in the placebo group and 32% in the nabilone group). There were no serious AEs.
Interpretation: Our results highlight the potential efficacy of nabilone for patients with PD with disturbing NMS, which appears to be driven by positive effects on anxious mood and night-time sleep problems.
Trial registry: ClinicalTrials.gov (NCT03769896) and EudraCT (2017-000192-86). ANN NEUROL 2020;88:712-722.
© 2020 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
M.P. received travel compensation for presentation of the study data after study end from AOP Orphan Pharmaceuticals AG, which manufactures the drug that is tested in this study. A.D. and B.H. received a travel grant from AOP Orphan Pharmaceuticals AG, which manufactures the study drug. K.K. is an employee at AOP Orphan Pharmaceuticals AG, which manufactured the study drug. K.S. reports personal fees from AOP Orphan Pharmaceuticals AG that manufactures the drug tested in this study. F.K., H.G.K., M.W., F.C., P.E., K.M., D.V., H.S., G.G., H.U., H.K., G.K.W., R.S., and W.P. have no conflict of interest to report.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
