

Anticoagulation Type and Early Recurrence in Cardioembolic Stroke: The IAC Study
- PMID: 32757753
- PMCID: PMC7484360
- DOI: 10.1161/STROKEAHA.120.028867
Anticoagulation Type and Early Recurrence in Cardioembolic Stroke: The IAC Study
Abstract
Background and purpose: In patients with acute ischemic stroke and atrial fibrillation, treatment with low molecular weight heparin increases early hemorrhagic risk without reducing early recurrence, and there is limited data comparing warfarin to direct oral anticoagulant (DOAC) therapy. We aim to compare the effects of the treatments above on the risk of 90-day recurrent ischemic events and delayed symptomatic intracranial hemorrhage.
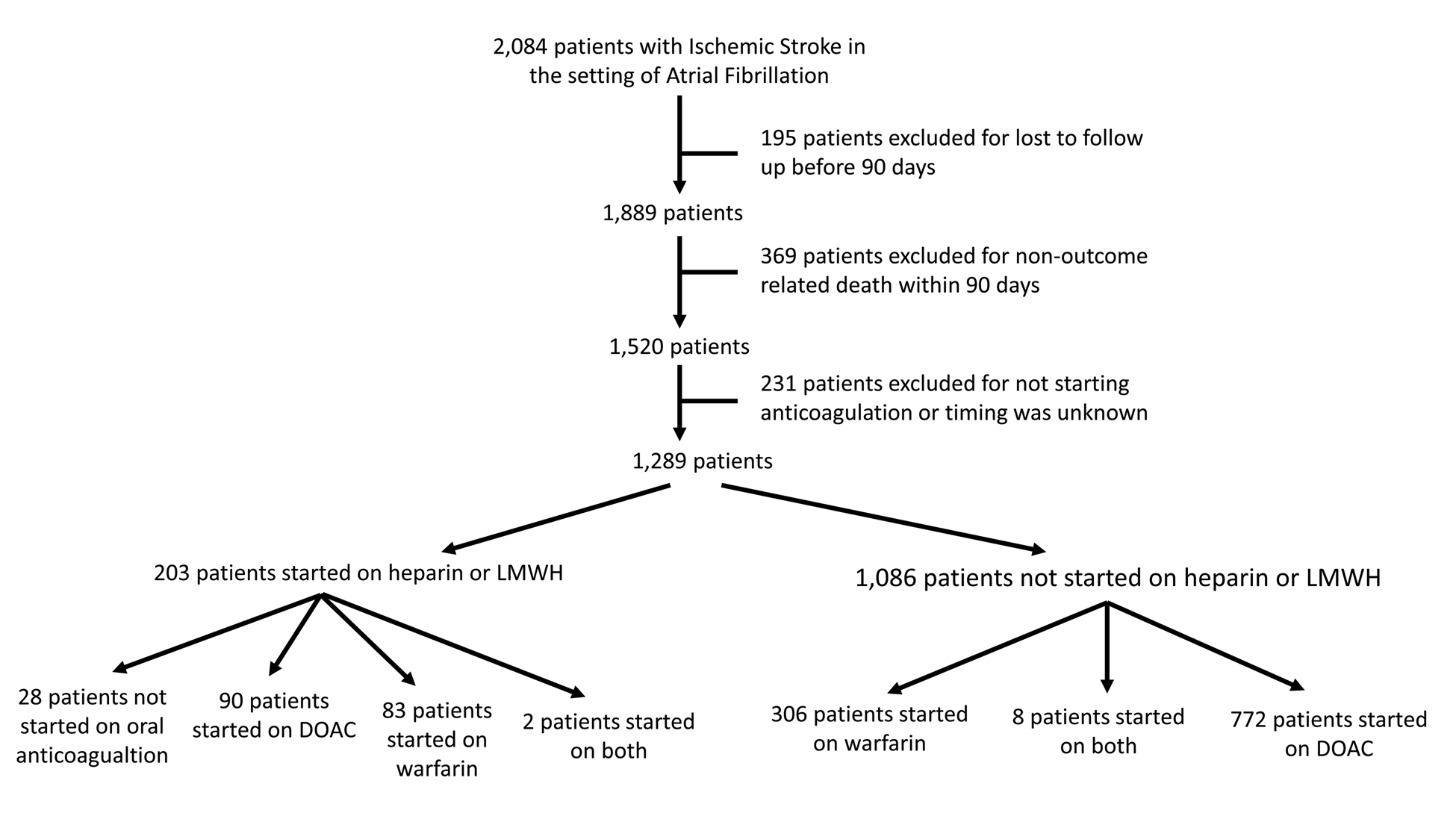
Methods: We included consecutive patients with acute ischemic stroke and atrial fibrillation from the IAC (Initiation of Anticoagulation after Cardioembolic) stroke study pooling data from stroke registries of 8 comprehensive stroke centers across the United States. We compared recurrent ischemic events and delayed symptomatic intracranial hemorrhage between each of the following groups in separate Cox-regression analyses: (1) DOAC versus warfarin and (2) bridging with heparin/low molecular weight heparin versus no bridging, adjusting for pertinent confounders to test these associations.
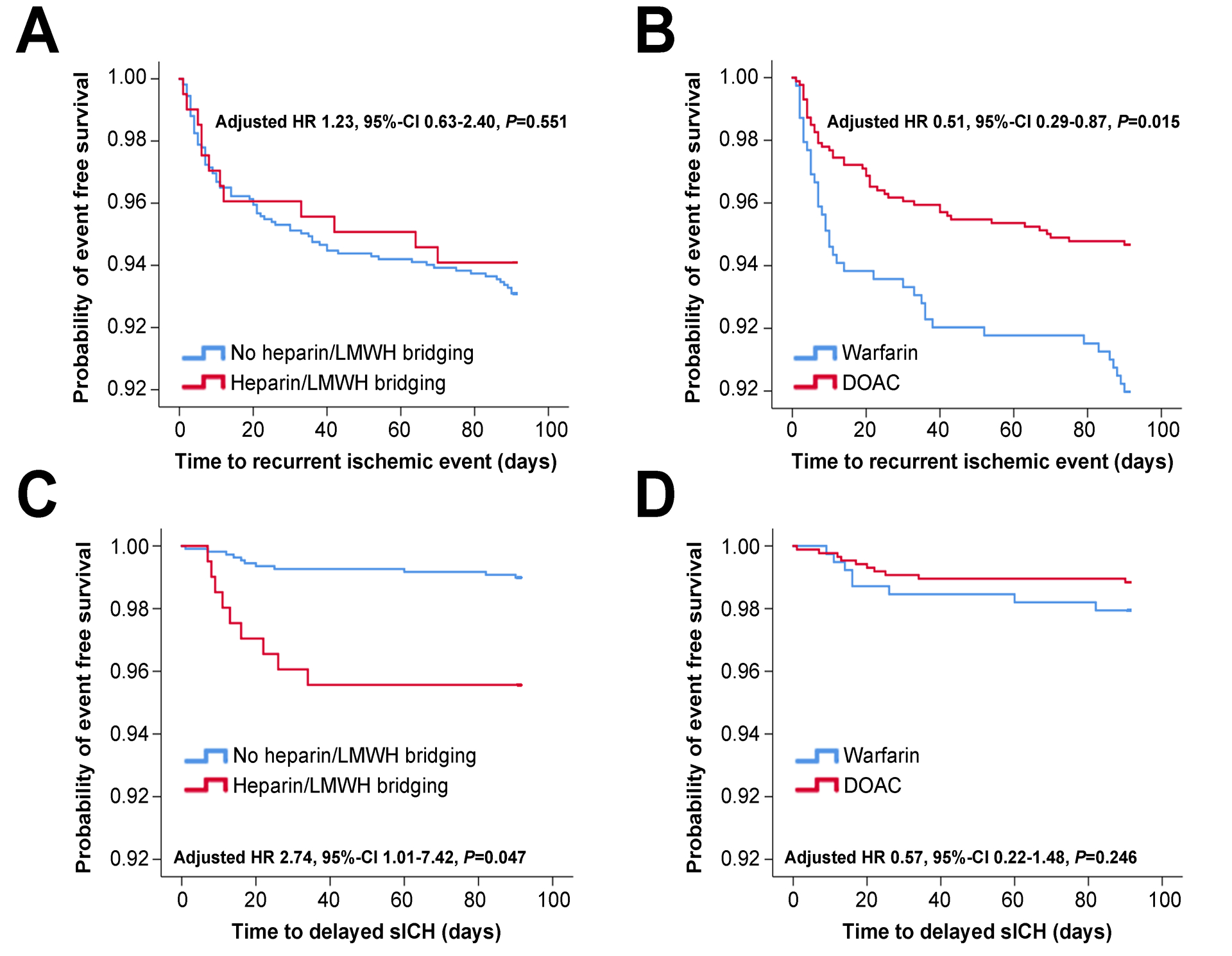
Results: We identified 1289 patients who met the bridging versus no bridging analysis inclusion criteria and 1251 patients who met the DOAC versus warfarin analysis inclusion criteria. In adjusted Cox-regression models, bridging (versus no bridging) treatment was associated with a high risk of delayed symptomatic intracranial hemorrhage (hazard ratio, 2.74 [95% CI, 1.01-7.42]) but a similar rate of recurrent ischemic events (hazard ratio, 1.23 [95% CI, 0.63-2.40]). Furthermore, DOAC (versus warfarin) treatment was associated with a lower risk of recurrent ischemic events (hazard ratio, 0.51 [95% CI, 0.29-0.87]) but not delayed symptomatic intracranial hemorrhage (hazard ratio, 0.57 [95% CI, 0.22-1.48]).
Conclusions: Our study suggests that patients with ischemic stroke and atrial fibrillation would benefit from the initiation of a DOAC without bridging therapy. Due to our study limitations, these findings should be interpreted with caution pending confirmation from large prospective studies.
Keywords: anticoagulant; atrial fibrillation; hemorrhage; heparin; warfarin.
Figures
Comment in
-
Art of Anticoagulation After Recent Ischemic Stroke.Stroke. 2020 Sep;51(9):2618-2619. doi: 10.1161/STROKEAHA.120.030997. Epub 2020 Aug 6. Stroke. 2020. PMID: 32757754 No abstract available.
References
-
- Arboix A, Garcia-Eroles L, Oliveres M, Massons JB, Targa C. Clinical predictors of early embolic recurrence in presumed cardioembolic stroke. Cerebrovascular diseases (Basel, Switzerland). 1998;8:345–353 - PubMed
-
- Berge E, Abdelnoor M, Nakstad PH, Sandset PM. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: A double-blind randomised study. Haest study group. Heparin in acute embolic stroke trial. Lancet (London, England). 2000;355:1205–1210 - PubMed
-
- England TJ, Bath PM, Sare GM, Geeganage C, Moulin T, O’Neill D, et al. Asymptomatic hemorrhagic transformation of infarction and its relationship with functional outcome and stroke subtype: Assessment from the tinzaparin in acute ischaemic stroke trial. Stroke. 2010;41:2834–2839 - PubMed
-
- Yaghi S, Willey JZ, Cucchiara B, Goldstein JN, Gonzales NR, Khatri P, et al. Treatment and outcome of hemorrhagic transformation after intravenous alteplase in acute ischemic stroke: A scientific statement for healthcare professionals from the american heart association/american stroke association. Stroke. 2017;48:e343–e361 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
