

Dabrafenib and Trametinib in Patients With Tumors With BRAFV600E Mutations: Results of the NCI-MATCH Trial Subprotocol H
- PMID: 32758030
- PMCID: PMC7676884
- DOI: 10.1200/JCO.20.00762
Dabrafenib and Trametinib in Patients With Tumors With BRAFV600E Mutations: Results of the NCI-MATCH Trial Subprotocol H
Abstract
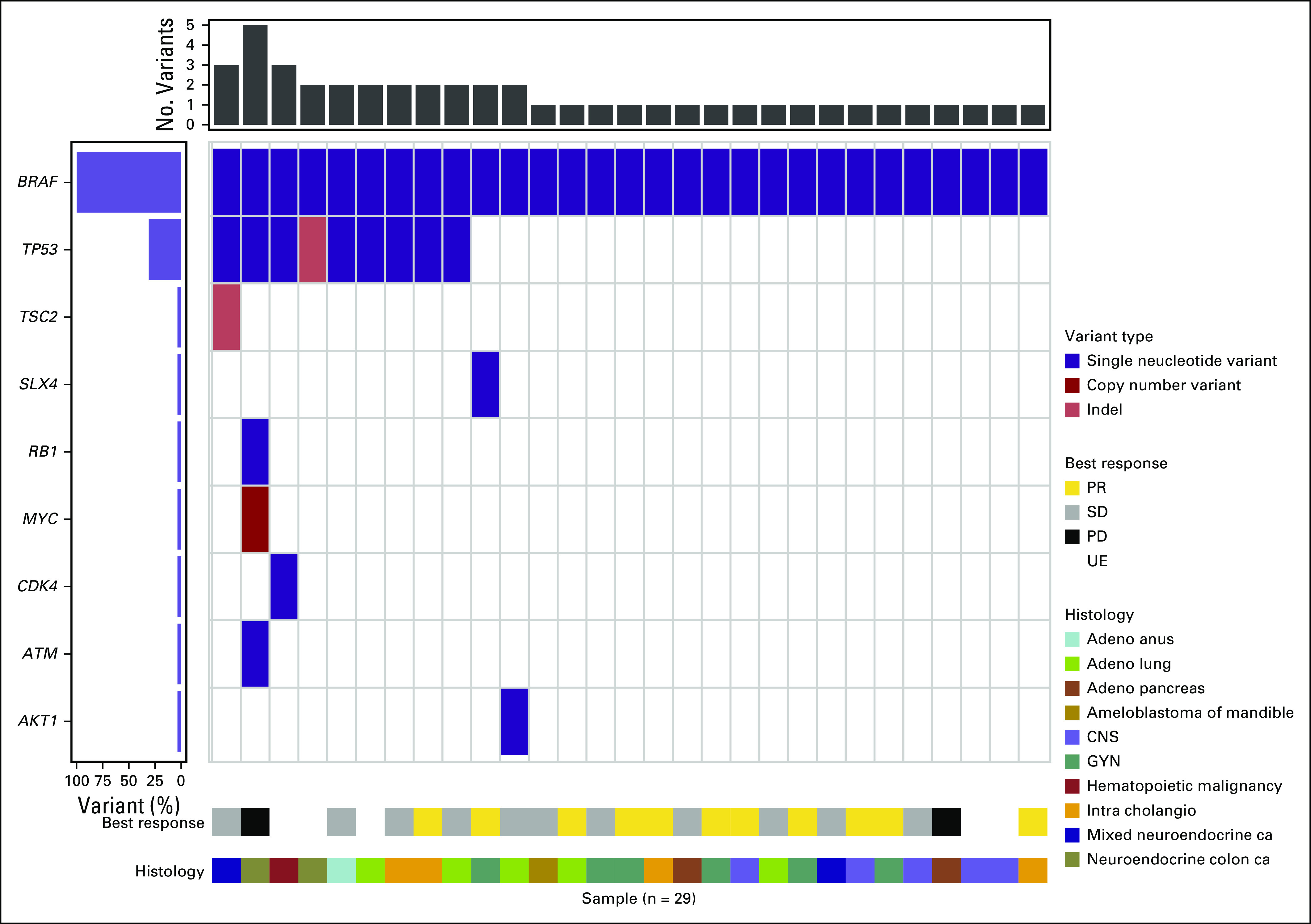
Purpose: BRAFV600 mutations are commonly found in melanoma and thyroid cancers and to a lesser degree in other tumor types. Subprotocol H (EAY131-H) of the NCI-MATCH platform trial sought to investigate the selective BRAF inhibitor dabrafenib and the MEK1/2 inhibitor trametinib in patients with solid tumors, lymphomas, or multiple myeloma whose tumors harbored a BRAFV600 mutation.
Patients and methods: EAY131-H is an open-label, single-arm study. Patients with melanoma, thyroid, or colorectal cancer were excluded; patients with non-small-cell lung cancer were later excluded in an amendment. Patients received dabrafenib 150 mg twice per day and trametinib 2 mg per day continuously until disease progression or intolerable toxicity. The primary end point was centrally assessed objective response rate (ORR); secondary end points included progression-free survival (PFS), 6-month PFS, and overall survival.
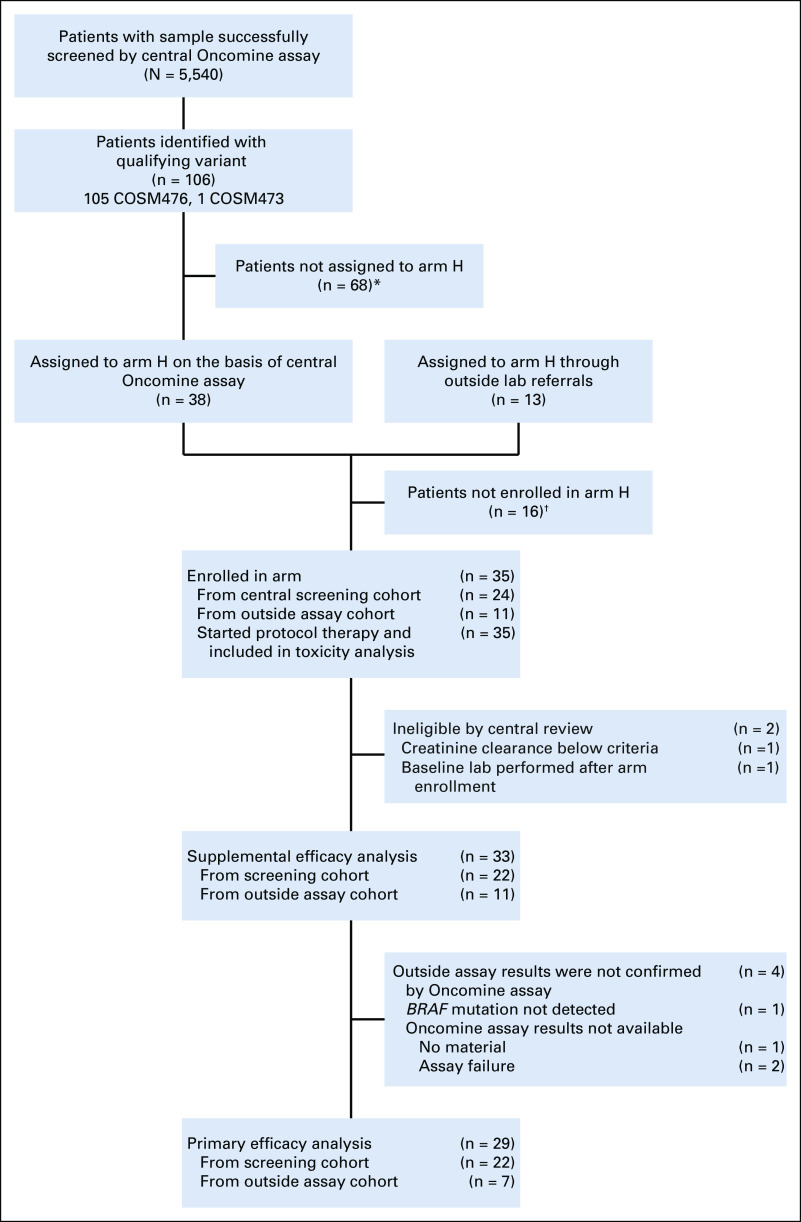
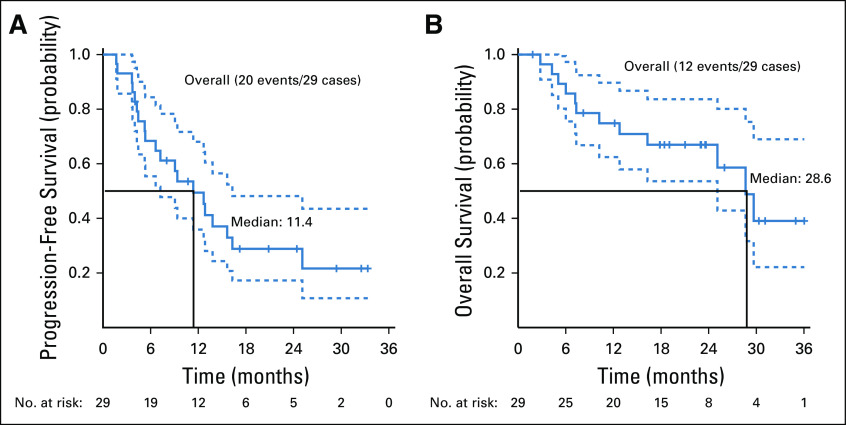
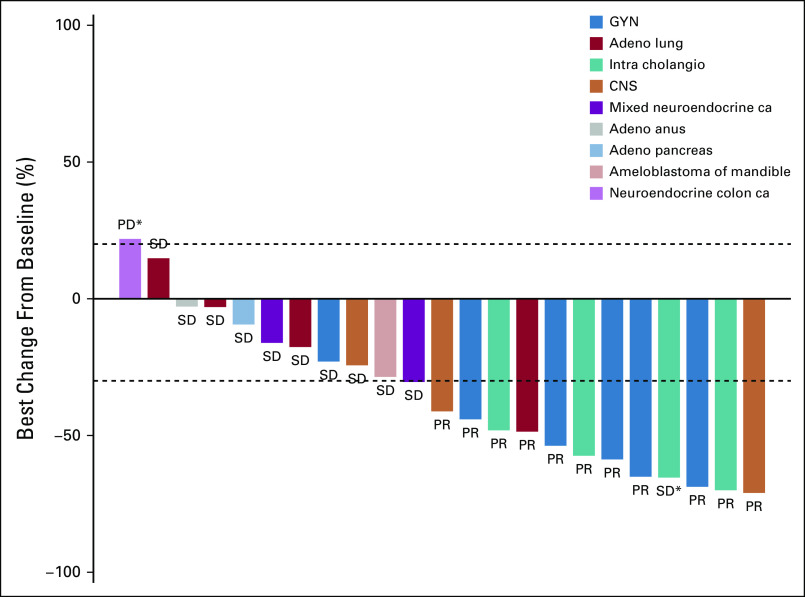
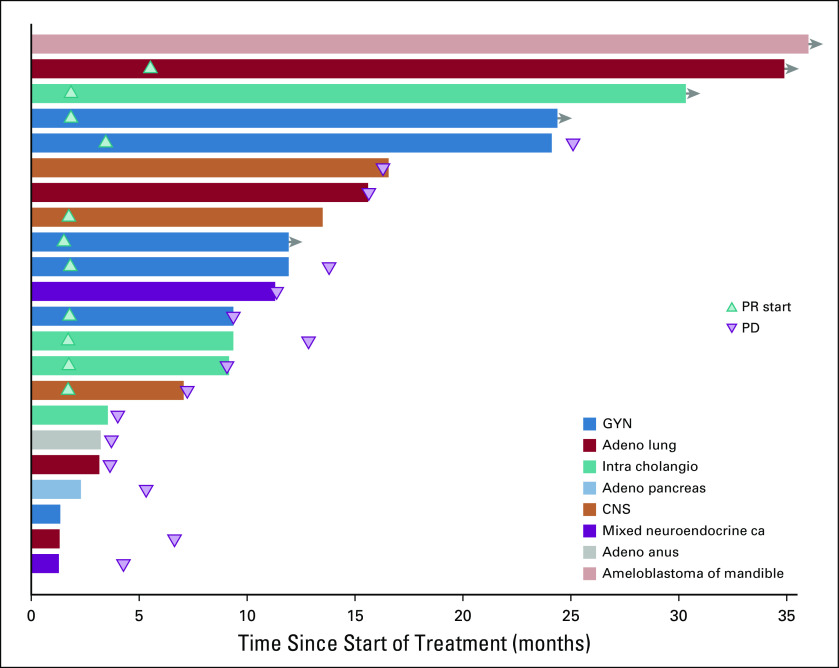
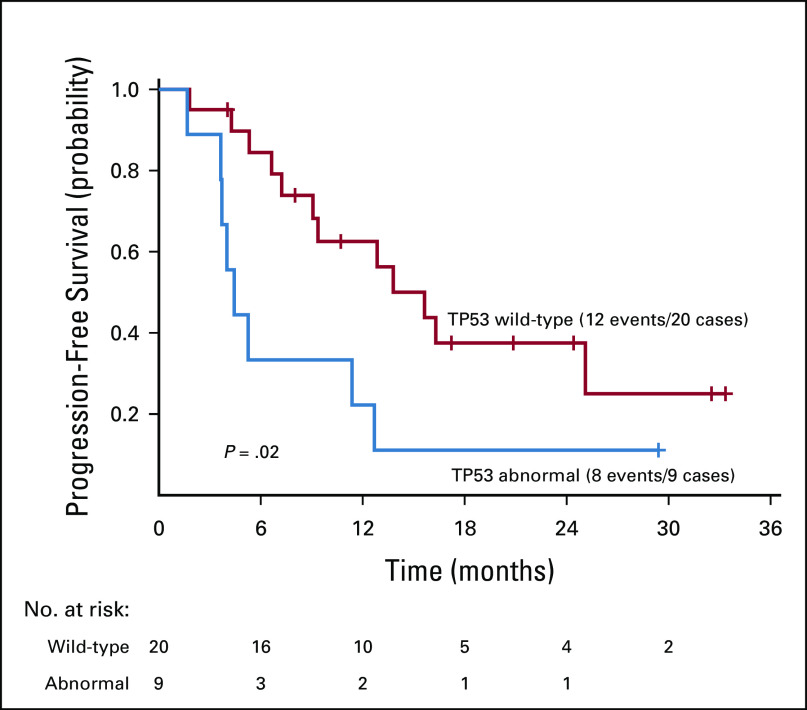
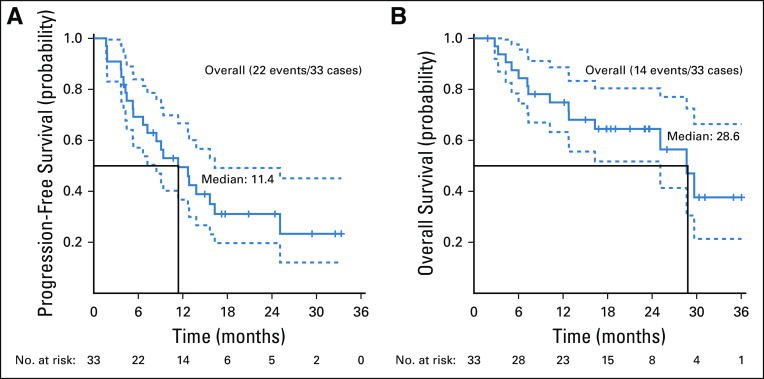
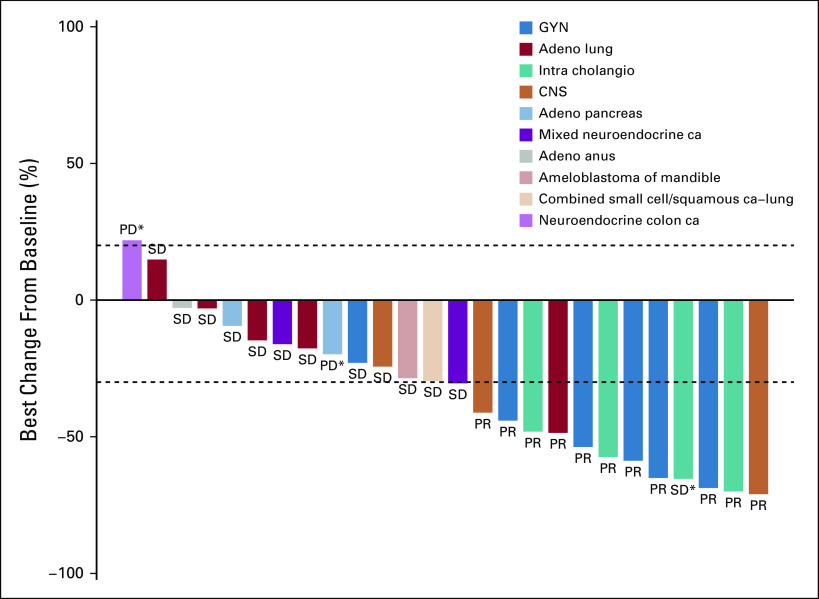
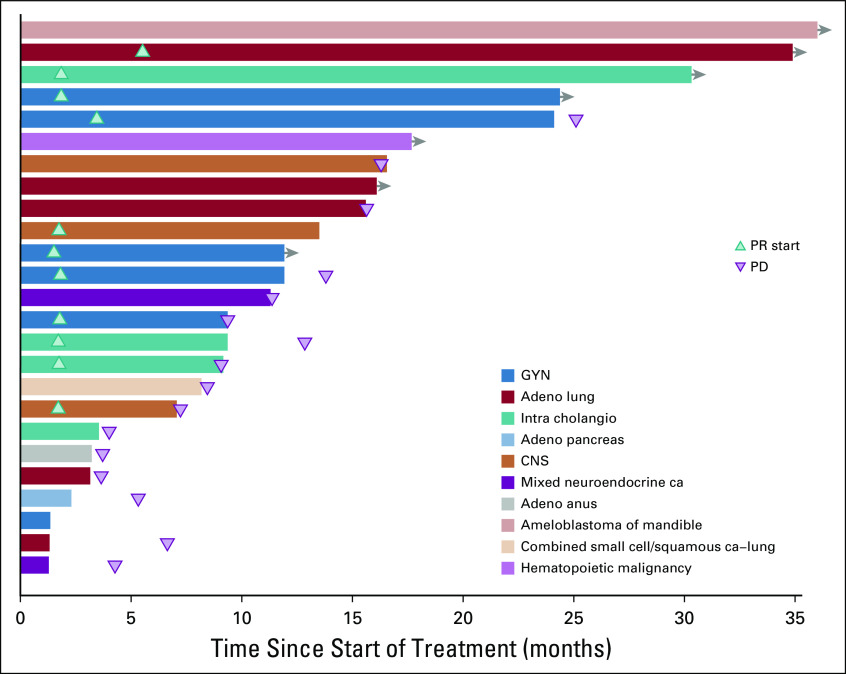
Results: Thirty-five patients were enrolled, and 29 were included in the primary efficacy analysis as prespecified in the protocol. Median age was 59 years, and 45% of the patients had received ≥ 3 lines of therapy. The confirmed ORR was 38% (90% CI, 22.9% to 54.9%) with P < .0001 against a null rate of 5%, and PFS was 11.4 months (90% CI, 8.4 to 16.3 months); responses were seen in 7 distinct tumor types. Seven patients had a duration of response of > 12 months, including 4 patients with a duration of response of > 24 months. An additional 8 patients had a PFS > 6 months. The median overall survival was 28.6 months. Reported adverse events were comparable to those noted in previously reported profiles of dabrafenib and trametinib.
Conclusion: This study met its primary end point, with an ORR of 38% (P < .0001) in this mixed histology, pretreated cohort. This promising activity warrants additional investigations in BRAFV600-mutated tumors outside of currently approved indications.
Conflict of interest statement
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, nor does mention of trade names, commercial products, or organizations imply endorsement by the US government.
Figures
References
-
- Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–954. - PubMed
-
- Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372:30–39. - PubMed
-
- Planchard D, Smit EF, Groen HJM, et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017;18:1307–1316. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
