

Clinical impact of PSMA PET/CT in primary prostate cancer compared to conventional nodal and distant staging: a retrospective single center study
- PMID: 32758168
- PMCID: PMC7409439
- DOI: 10.1186/s12885-020-07192-7
Clinical impact of PSMA PET/CT in primary prostate cancer compared to conventional nodal and distant staging: a retrospective single center study
Abstract
Background: To evaluate the impact of Gallium-68 [68Ga] labeled prostate specific membrane antigen (PSMA) positron emission tomography (PET)/X-ray computed tomography (CT) compared with conventional imaging on staging and clinical management of men evaluated for primary prostate cancer (PCa).
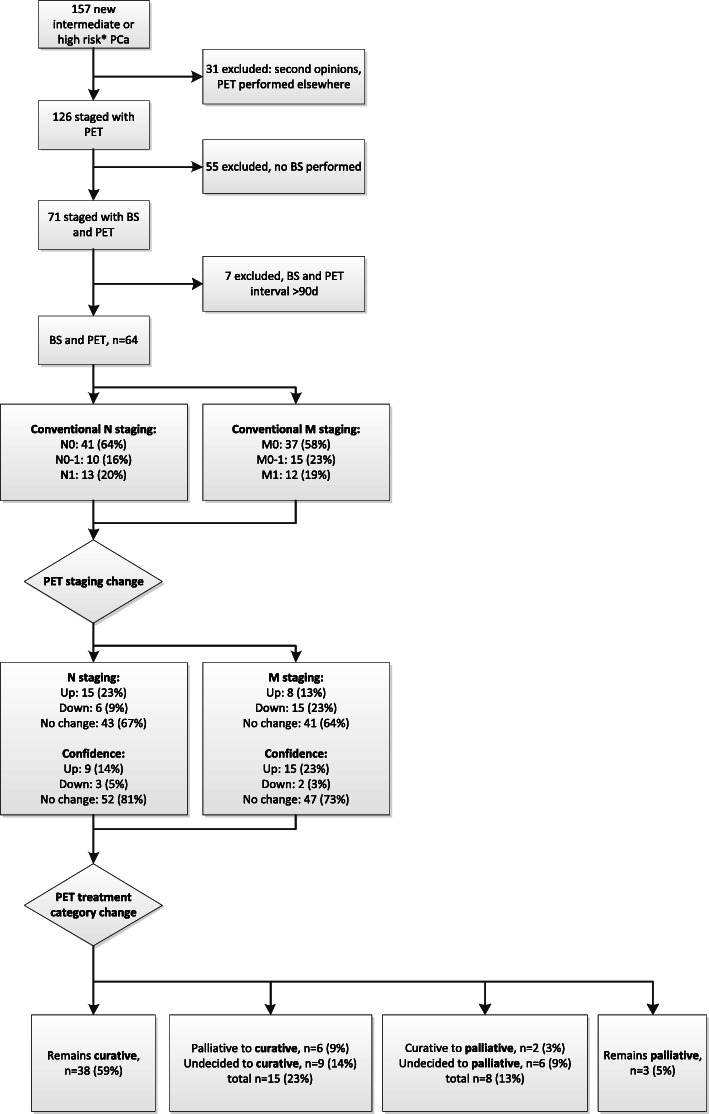
Methods: Men with newly diagnosed biopsy-proven PCa who had been staged with a conventional staging protocol including bone scintigraphy (BS) and additionally underwent [68Ga]PSMA PET/CT, were evaluated retrospectively. Imaging findings from BS, magnetic resonance imaging (MRI) and/or CT were categorized regarding locoregional nodal (N) and distant metastasis (M) status as negative, positive or equivocal before and after addition of the information of PET/CT. Also, the imaging-based level of confidence (LoC) in correct assessment of N and M status was scored. Impact of PET/CT on clinical management was evaluated by the percentage of treatment category changes after PET/CT as determined in the multidisciplinary tumour board.
Results: Sixty-four men with intermediate and high-risk PCa were evaluated. With additional information of PET/CT, N status was upstaged in 23%, and downstaged in 9%. M status was upstaged in 13%, and downstaged in 23%. A net increase in LoC of 20% was noted, mainly regarding M status. Treatment category changed from palliative to curative in 9%, and from curative to palliative in 3%. An undecided treatment plan changed to curative in 14%, as well as to palliative in another 9%. In total, a 36% treatment category change was noted. High negative predictive value of PET/CT for M status was indicated by 27 patients that underwent robot-assisted radical prostatectomy and reached postoperative biochemical disease-free status or had a likely other site of disease recurrence.
Conclusions: PSMA PET/CT can cause considerable changes in N and M staging, as well as in management compared to conventional staging. Findings of this study support the replacement of BS and CT by PSMA PET/CT in staging primary PCa.
Keywords: Impact; Management; PSMA; Prostate; Staging.
Conflict of interest statement
None.
Figures
References
-
- Gordon LG, Tuffaha HW, James R, Keller AT, Lowe A, Scuffham PA, et al. Estimating the healthcare costs of treating prostate cancer in Australia: a Markov modelling analysis. Urol Oncol. 2018;36(3):91 e7–91e15. - PubMed
-
- Mottet N, van den Bergh RCN, Briers E, Comford P, De Santis S, Gillessen S, et al. Prostate cancer. Arnhem: EAU Guidelines Office; 2019.
-
- Janssen JC, Meissner S, Woythal N, Prasad V, Brenner W, Diederichs G, et al. Comparison of hybrid (68) Ga-PSMA-PET/CT and (99m) Tc-DPD-SPECT/CT for the detection of bone metastases in prostate cancer patients: additional value of morphologic information from low dose CT. Eur Radiol. 2018;28(2):610–619. - PubMed
-
- Pyka T, Okamoto S, Dahlbender M, Tauber R, Retz M, Heck M, et al. Comparison of bone scintigraphy and (68)Ga-PSMA PET for skeletal staging in prostate cancer. Eur J Nucl Med Mol Imaging. 2016;43(12):2114–2121. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
