

Reducing Inpatient Hypoglycemia in the General Wards Using Real-time Continuous Glucose Monitoring: The Glucose Telemetry System, a Randomized Clinical Trial
- PMID: 32759361
- PMCID: PMC7576426
- DOI: 10.2337/dc20-0840
Reducing Inpatient Hypoglycemia in the General Wards Using Real-time Continuous Glucose Monitoring: The Glucose Telemetry System, a Randomized Clinical Trial
Abstract
Objective: Use of real-time continuous glucose monitoring (RT-CGM) systems in the inpatient setting is considered investigational. The objective of this study was to evaluate whether RT-CGM, using the glucose telemetry system (GTS), can prevent hypoglycemia in the general wards.
Research design and methods: In a randomized clinical trial, insulin-treated patients with type 2 diabetes at high risk for hypoglycemia were recruited. Participants were randomized to RT-CGM/GTS or point-of-care (POC) blood glucose testing. The primary outcome was difference in inpatient hypoglycemia.
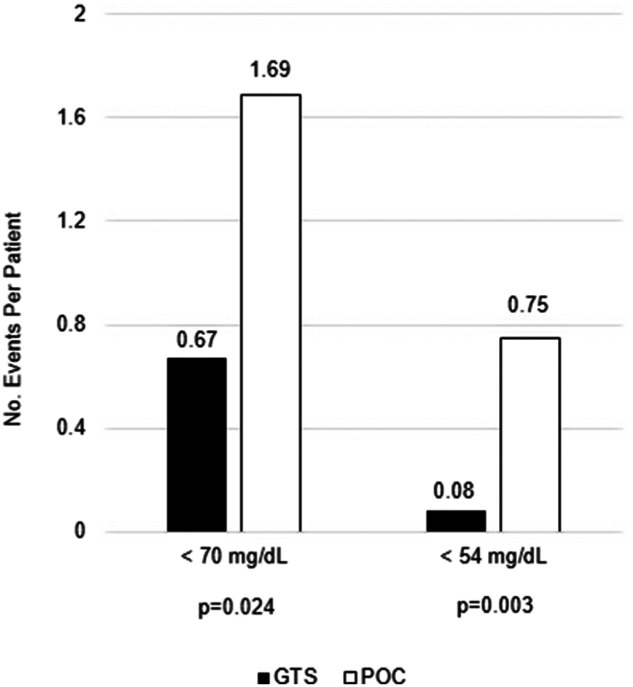
Results: Seventy-two participants were included in this interim analysis, 36 in the RT-CGM/GTS group and 36 in the POC group. The RT-CGM/GTS group experienced fewer hypoglycemic events (<70 mg/dL) per patient (0.67 [95% CI 0.34-1.30] vs. 1.69 [1.11-2.58], P = 0.024), fewer clinically significant hypoglycemic events (<54 mg/dL) per patient (0.08 [0.03-0.26] vs. 0.75 [0.51-1.09], P = 0.003), and a lower percentage of time spent below range <70 mg/dL (0.40% [0.18-0.92%] vs. 1.88% [1.26-2.81%], P = 0.002) and <54 mg/dL (0.05% [0.01-0.43%] vs. 0.82% [0.47-1.43%], P = 0.017) compared with the POC group. No differences in nocturnal hypoglycemia, time in range 70-180 mg/dL, and time above range >180-250 mg/dL and >250 mg/dL were found between the groups. The RT-CGM/GTS group had no prolonged hypoglycemia compared with 0.20 episodes <54 mg/dL and 0.40 episodes <70 mg/dL per patient in the POC group.
Conclusions: RT-CGM/GTS can decrease hypoglycemia among hospitalized high-risk insulin-treated patients with type 2 diabetes.
© 2020 by the American Diabetes Association.
Figures

Comment on
-
The Impact of COVID-19 on CGM Use in the Hospital.Diabetes Care. 2020 Nov;43(11):2628-2630. doi: 10.2337/dci20-0046. Epub 2020 Sep 25. Diabetes Care. 2020. PMID: 32978180 No abstract available.
References
-
- Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 2002;87:978–982 - PubMed
-
- McAlister FA, Man J, Bistritz L, Amad H, Tandon P. Diabetes and coronary artery bypass surgery: an examination of perioperative glycemic control and outcomes. Diabetes Care 2003;26:1518–1524 - PubMed
-
- Akirov A, Diker-Cohen T, Masri-Iraqi H, Shimon I. High glucose variability increases mortality risk in hospitalized patients. J Clin Endocrinol Metab 2017;102:2230–2241 - PubMed
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
