

A Single Liver Metastasis from Pleural Biphasic Mesothelioma
- PMID: 32759747
- PMCID: PMC7460021
- DOI: 10.3390/diagnostics10080555
A Single Liver Metastasis from Pleural Biphasic Mesothelioma
Abstract
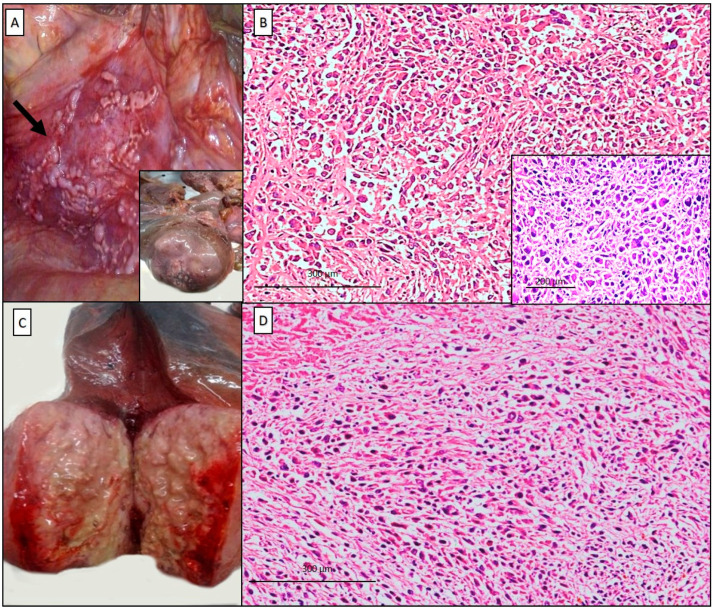
Virtually any malignancy can metastasize to the liver. Large solitary metastases are rare and can be difficult to distinguish from primary tumors. Malignant mesothelioma is often considered as a locally invasive cancer but tumor dissemination to extra-thoracic sites is possible, and the liver can be involved. Herein, we present a rare case of pleural mesothelioma with a solitary large liver metastasis diagnosed postmortem in a ninety-two-year-old man with 35 years of exposure to asbestos. Results of immunohistochemical staining of the pleural and liver tumor were similar, both positive for low-molecular weight keratins, calretinin, vimentin, and podoplanin, and negative for Claudin-4, TTF1, CEA, BerEP4, CK7, CK19, CK20, BAP1, Hep Par1, p40, and WT1. Fluorescent in-situ hybridization (FISH) for p16/CDKN2A was also performed and a homozygous deletion was detected in both tumors, supporting the diagnosis of mesothelioma. Reporting this case, we would like to point out that extra-thoracic dissemination from pleural mesothelioma, even if exceptional, can occur. In cases where differential diagnoses are challenging, the value of ancillary techniques and a practical approach to diagnostic work-up is of primary importance.
Keywords: asbestos exposure; autopsy; liver; malignant pleural mesothelioma; metastasis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- International Agency for Research on Cancer (IARC) WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. World Health Organization; Lyon, France: 2015.
-
- Husain A.N., Colby T.V., Ordóñez N.G., Allen T.C., Attanoos R.L., Beasley M.B., Butnor K.J., Chirieac L.R., Churg A.M., Dacic S., et al. Guidelines for Pathologic Diagnosis of Malignant Mesothelioma 2017 Update of the Consensus Statement From the International Mesothelioma Interest Group. Arch. Pathol. Lab. Med. 2018;142:89–108. doi: 10.5858/arpa.2017-0124-RA. - DOI - PubMed
-
- Vimercati L., Cavone D., Lovreglio P., De Maria L., Caputi A., Ferri G.M., Serio G. Environmental Asbestos Exposure And Mesothelioma Cases In Bari Apulia Region Southern Italy A National Interest Site For Land Reclamation. Environ. Sci. Pollut. R. 2018;25:15692–15701. doi: 10.1007/s11356-018-1618-x. - DOI - PMC - PubMed
-
- Serio G., Pezzuto F., Marzullo A., Scattone A., Cavone D., Punzi A., Fortarezza F., Gentile M., Buonadonna A.L., Barbareschi M., et al. Peritoneal mesothelioma with residential asbestos exposure. Report of a case with long survival (seventeen years) analyzed by Cgh-array. Int. J. Mol. Sci. 2017;18:1818. doi: 10.3390/ijms18081818. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
