

Impaired consciousness at stroke onset in large hemisphere infarction: incidence, risk factors and outcome
- PMID: 32759986
- PMCID: PMC7406648
- DOI: 10.1038/s41598-020-70172-1
Impaired consciousness at stroke onset in large hemisphere infarction: incidence, risk factors and outcome
Abstract
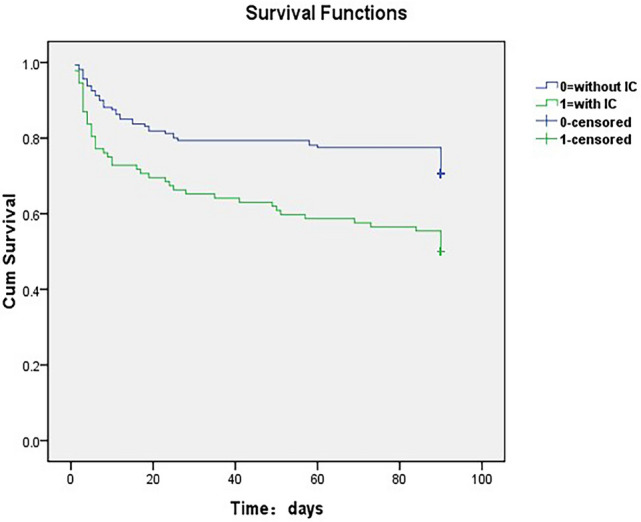
Impaired consciousness (IC) at stroke onset in large hemispheric infarctions (LHI) patients is common in clinical practice. However, little is known about the incidence and risk factors of IC at stroke onset in LHI. Besides, stroke-related complications and clinical outcomes in relation to the development of IC has not been systematically examined. Data of 256 consecutive patients with LHI were collected. IC at stroke onset was retrospectively collected from the initial emergency department and/or admission records. Of the 256 LHI patients enrolled, 93 (36.3%) had IC at stroke onset. LHI patients with IC at stroke onset were older (median age 66 vs. 61, p = 0.041), had shorter prehospital delay (24 vs. 26 h, p < 0.001and higher baseline National Institutes of Health Stroke Scale (NIHSS) score (19 vs. 12, p < 0.001). Independent risk factors of IC at stroke onset were high NIHSS score (odds ratio, OR 1.17, 95% confidence interval [CI] 1.12 to 1.23) and atrial fibrillation (OR 1.93, 95% CI 1.07 to 3.47). Dyslipidemia appeared to protect against IC at stroke onset (adjusted OR 0.416, 95% CI 0.175 to 0.988). IC at stroke onset was associated with higher frequency of stroke-related complications (90.32% vs. 67.48%, p < 0.001), especially brain edema (45.16% vs. 23.31%, p < 0.001) and pneumonia (63.44% vs. 47.82%, p = 0.019). The IC group had higher rates of in-hospital death (23.66% vs. 11.66%, p = 0.012), 3-month mortality (49.46% vs. 24.87%, p = 0.002), and 3-month unfavorable outcome (64.51% vs. 49.07%, p = 0.017). However, after adjusting for age, baseline NIHSS score and other confounders, IC at stroke onset was not an independent predictor of in-hospital death (adjusted OR 0.56, 95% CI 0.22 to 1.47), 3-month mortality (adjusted OR 0.54, 95% CI 0.25 to 1.14) and 3-month unfavorable outcome (adjusted OR 0.64, 95% CI 0.31 to 1.33) in LHI patients (all p > 0.05). Our results suggested that IC occur in 1 out of every 3 LHI patients at stroke onset and was associated with initial stroke severity and atrial fibrillation. LHI patients with IC at stroke onset more frequently had stroke-related complications, 3-month mortality and unfavorable outcome, whereas IC was not an independent predictor of poor outcomes.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Lai P-F, Yiang G-T, Tsai M-J, Hu S-C. Analysis of patients with altered mental status in an emergency Department of Eastern Taiwan. Tzu Chi Med. J. 2009;21:151–155.
-
- Levy DE, et al. Prognosis in nontraumatic coma. Ann. Intern. Med. 1981;94:293–301. - PubMed
-
- Melo TP, De Mendonca A, Crespo M, Carvalho M, Ferro JM. An emergency room-based study of stroke coma. Cerebrovasc. Dis. 1992;2:93–101.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
