

Classical Cesarean Section
- PMID: 32760792
- PMCID: PMC7396476
- DOI: 10.1055/s-0039-3402072
Classical Cesarean Section
Abstract
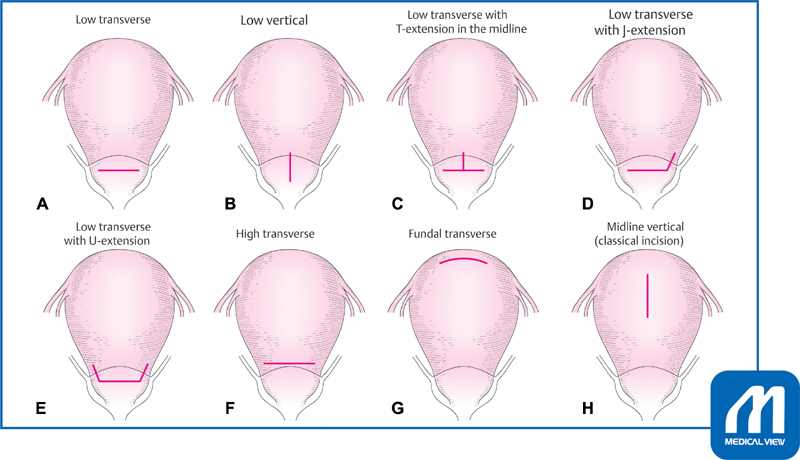
Cesarean section is the most common surgery in obstetrics. Several techniques are proposed according to the indication and the degree of urgency. Usually laparotomy followed by hysterotomy with a low transverse incision is preferable. However, in cases in which it is difficult to access the lower uterine segment, such as that in preterm labor, dense adhesion, placenta previa/accrete a vertical hysterotomy (classical cesarean section) may be needed. Although a smooth and gentle delivery of the fetus is possible through the vertical incision, uterine closure is technically difficult. To decrease the risks of hemorrhage and adhesion, a speedy and skillful technique is mandatory. The most serious risk of vertical incision in the contractile corpus is uterine rupture in the subsequent pregnancy. Therefore, cases of prior classical cesarean section are contraindicated for trial of labor after cesarean section.
Keywords: cesarean section; classical cesarean section; uterine rupture; vertical uterine incision.
Conflict of interest statement
Conflict of Interest None.
Figures



References
-
- Luthra G, Gawade P, Starikov R, Markenson G. Uterine incision-to-delivery interval and perinatal outcomes in transverse versus vertical incisions in preterm cesarean deliveries. J Matern Fetal Neonatal Med. 2013;26(18):1788–1791. - PubMed
-
- Patterson L S, O'Connell C M, Baskett T F. Maternal and perinatal morbidity associated with classic and inverted T cesarean incisions. Obstet Gynecol. 2002;100(04):633–637. - PubMed
-
- American College of Obstetricians and Gynecologists.ACOG practice bulletin. Vaginal birth after previous cesarean delivery. Number 5, July 1999 (replaces practice bulletin number 2, October 1998). Clinical management guidelines for obstetrician-gynecologists Int J Gynaecol Obstet 19996602197–204. - PubMed
-
- Shipp T D, Zelop C M, Repke J T, Cohen A, Caughey A B, Lieberman E.Intrapartum uterine rupture and dehiscence in patients with prior lower uterine segment vertical and transverse incisions Obstet Gynecol 199994(5 Pt 1):735–740. - PubMed
-
- Halperin M E, Moore D C, Hannah W J. Classical versus low-segment transverse incision for preterm caesarean section: maternal complications and outcome of subsequent pregnancies. Br J Obstet Gynaecol. 1988;95(10):990–996. - PubMed
LinkOut - more resources
Full Text Sources