

Efficacy of Ketogenic Diet, Modified Atkins Diet, and Low Glycemic Index Therapy Diet Among Children With Drug-Resistant Epilepsy: A Randomized Clinical Trial
- PMID: 32761191
- PMCID: PMC7400196
- DOI: 10.1001/jamapediatrics.2020.2282
Efficacy of Ketogenic Diet, Modified Atkins Diet, and Low Glycemic Index Therapy Diet Among Children With Drug-Resistant Epilepsy: A Randomized Clinical Trial
Abstract
Importance: The ketogenic diet (KD) has been used successfully to treat children with drug-resistant epilepsy. Data assessing the efficacy of the modified Atkins diet (MAD) and low glycemic index therapy (LGIT) diet compared with the KD are scarce.
Objective: To determine whether the MAD and LGIT diet are noninferior to the KD among children with drug-resistant epilepsy.
Design, setting, and participants: One hundred seventy children aged between 1 and 15 years who had 4 or more seizures per month, had not responded to 2 or more antiseizure drugs, and had not been treated previously with the KD, MAD, or LGIT diet were enrolled between April 1, 2016, and August 20, 2017, at a tertiary care referral center in India.
Exposures: Children were randomly assigned to receive the KD, MAD, or LGIT diet as additions to ongoing therapy with antiseizure drugs.
Main outcomes and measures: Primary outcome was percentage change in seizure frequency after 24 weeks of dietary therapy in the MAD cohort compared with the KD cohort and in the LGIT diet cohort compared with the KD cohort. The trial was powered to assess noninferiority of the MAD and LGIT diet compared with the KD with a predefined, noninferiority margin of -15 percentage points. Intention-to-treat analysis was used.
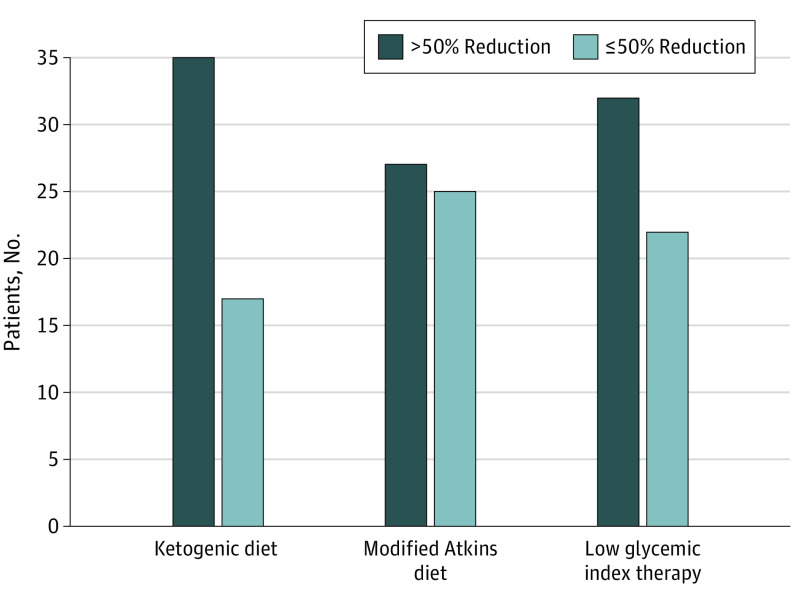
Results: One hundred fifty-eight children completed the trial: KD (n = 52), MAD (n = 52), and LGIT diet (n = 54). Intention-to-treat analysis showed that, after 24 weeks of intervention, the median (interquartile range [IQR]) change in seizure frequency (KD: -66%; IQR, -85% to -38%; MAD: -45%; IQR, -91% to -7%; and LGIT diet: -54%; IQR, -92% to -19%) was similar among the 3 arms (P = .39). The median difference, per intention-to-treat analysis, in seizure reduction between the KD and MAD arms was -21 percentage points (95% CI, -29 to -3 percentage points) and between the KD and LGIT arms was -12 percentage points (95% CI, -21 to 7 percentage points), with both breaching the noninferiority margin of -15 percentage points. Treatment-related adverse events were similar between the KD (31 of 55 [56.4%]) and MAD (33 of 58 [56.9%]) arms but were significantly less in the LGIT diet arm (19 of 57 [33.3%]).
Conclusions and relevance: Neither the MAD nor the LGIT diet met the noninferiority criteria. However, the results of this study for the LGIT diet showed a balance between seizure reduction and relatively fewer adverse events compared with the KD and MAD. These potential benefits suggest that the risk-benefit decision with regard to the 3 diet interventions needs to be individualized.
Trial registration: ClinicalTrials.gov Identifier: NCT02708030.
Conflict of interest statement
Figures

Comment in
-
Efficacy of 3 Major Ketogenic Diet Therapies in Children With Drug-Resistant Epilepsy-Reply.JAMA Pediatr. 2021 Apr 1;175(4):434-435. doi: 10.1001/jamapediatrics.2020.5451. JAMA Pediatr. 2021. PMID: 33492336 No abstract available.
-
Efficacy of 3 Major Ketogenic Diet Therapies in Children With Drug-Resistant Epilepsy.JAMA Pediatr. 2021 Apr 1;175(4):434. doi: 10.1001/jamapediatrics.2020.5448. JAMA Pediatr. 2021. PMID: 33492351 No abstract available.
References
-
- Kossoff EH, Zupec-Kania BA, Auvin S, et al. ; Charlie Foundation; Matthew’s Friends; Practice Committee of the Child Neurology Society . Optimal clinical management of children receiving dietary therapies for epilepsy: updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open. 2018;3(2):175-192. doi:10.1002/epi4.12225 - DOI - PMC - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
