

Acute Stroke Presentation, Care, and Outcomes in Community Hospitals in Northern California During the COVID-19 Pandemic
- PMID: 32762619
- PMCID: PMC7434008
- DOI: 10.1161/STROKEAHA.120.031099
Acute Stroke Presentation, Care, and Outcomes in Community Hospitals in Northern California During the COVID-19 Pandemic
Abstract
Background and purpose: Shelter-in-place (SIP) orders implemented to mitigate severe acute respiratory syndrome coronavirus 2 spread may inadvertently discourage patient care-seeking behavior for critical conditions like acute ischemic stroke. We aimed to compare temporal trends in volume of acute stroke alerts, patient characteristics, telestroke care, and short-term outcomes pre- and post-SIP orders.
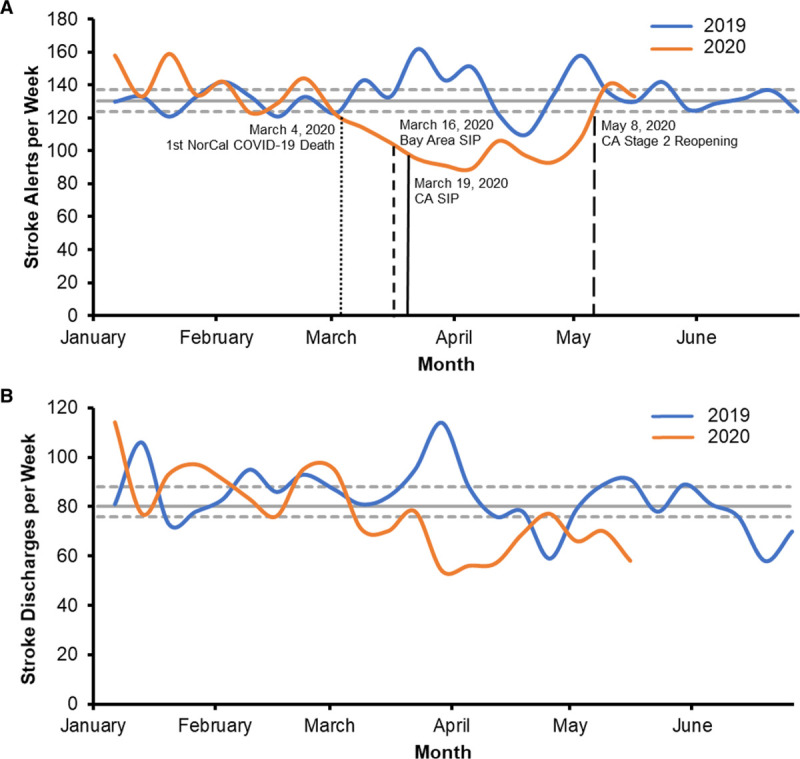
Methods: We conducted a cohort study in 21 stroke centers of an integrated healthcare system serving 4.4+ million members across Northern California. We included adult patients who presented with suspected acute stroke and were evaluated by telestroke between January 1, 2019, and May 9, 2020. SIP orders announced the week of March 15, 2020, created pre (January 1, 2019, to March 14, 2020) and post (March 15, 2020, to May 9, 2020) cohort for comparison. Main outcomes were stroke alert volumes and inpatient mortality for stroke.
Results: Stroke alert weekly volume post-SIP (mean, 98 [95% CI, 92-104]) decreased significantly compared with pre-SIP (mean, 132 [95% CI, 130-136]; P<0.001). Stroke discharges also dropped, in concordance with acute stroke alerts decrease. In total, 9120 patients were included: 8337 in pre- and 783 in post-SIP cohorts. There were no differences in patient demographics. Compared with pre-SIP, post-SIP patients had higher National Institutes of Health Stroke Scale scores (P=0.003), lower comorbidity score (P<0.001), and arrived more often by ambulance (P<0.001). Post-SIP, more patients had large vessel occlusions (P=0.03), and there were fewer stroke mimics (P=0.001). Discharge outcomes were similar for post-SIP and pre-SIP cohorts.
Conclusions: In this cohort study, regional stroke alert and ischemic stroke discharge volumes decreased significantly in the early COVID-19 pandemic. Compared with pre-SIP, the post-SIP population showed no significant demographic differences but had lower comorbidity scores, more severe strokes, and more large vessel occlusions. The inpatient mortality was similar in both cohorts. Further studies are needed to understand the causes and implications of care avoidance to patients and healthcare systems.
Keywords: cohort studies; coronavirus; inpatients; patient care; stroke.
Figures
References
-
- Coronavirus Disease 2019 (COVID-19) - Cases in the US. Centers for Disease Control and Prevention; https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html.... Accessed June 25, 2020.
-
- World Health Organization; WHO Coronavirus Disease (COVID-19) Dashboard. https://covid19.who.int/. Accessed June 25, 2020.
-
- Rosenbaum L. The untold toll - the pandemic’s effects on patients without Covid-19. N Engl J Med. 2020; 382:2368–2371doi: 10.1056/NEJMms2009984 - PubMed
